CT: computed tomography; ICU: intensive care unit; IHCA: in-hospital cardiac arrest; IVS: interventricular septum; TAVI: transcatheter aortic valve implantation; TOE: transoesophageal echocardiogram; VSD: ventricular septal defect
Learning objectives
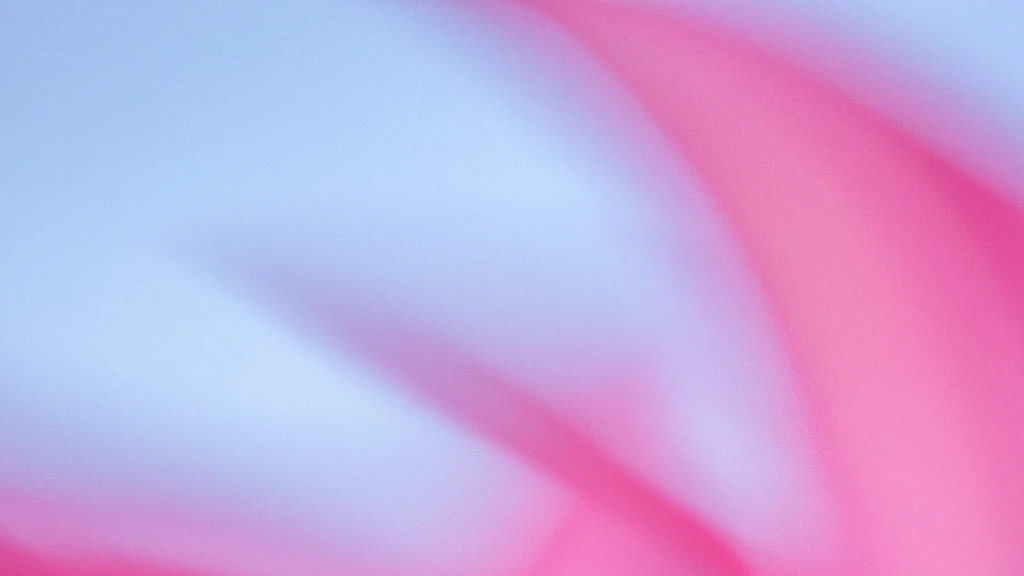
- Iatrogenic VSD after TAVI is a rare but serious complication.
- Management depends on the VSD size and haemodynamic impact and should be patient-tailored.
- Percutaneous transcatheter closure is feasible as a bailout in inoperable patients but may lead to further complications, i.e., mechanical haemolysis.
Iatrogenic ventricular septal defect (VSD) following transcatheter aortic valve implantation (TAVI) is a rare but serious complication, particularly associated with the use of balloon-expandable prostheses, with an estimated incidence of less than 1%.12 If untreated, haemodynamically significant shunts may lead to progressive heart failure and are associated with high mortality.1 However, both percutaneous and surgical treatment strategies have demonstrated favourable outcomes when performed successfully.134567 We present a case of right ventricular failure caused by a left-to-right shunt secondary to an iatrogenic VSD after TAVI, which was successfully treated with percutaneous VSD occluder implantation. The report focuses on imaging diagnostics, the clinical decision-making process, and key aspects of the interventional technique.
Case presentation
An 80-year-old male patient was admitted to our hospital for elective TAVI due to symptomatic severe aortic stenosis (AS). His medical history included chronic heart failure with a reduced left ventricular ejection fraction of 35% secondary to post-myocarditis dilated cardiomyopathy, as well as type 2 diabetes mellitus on oral medication, arterial hypertension, and chronic obstructive pulmonary disease.
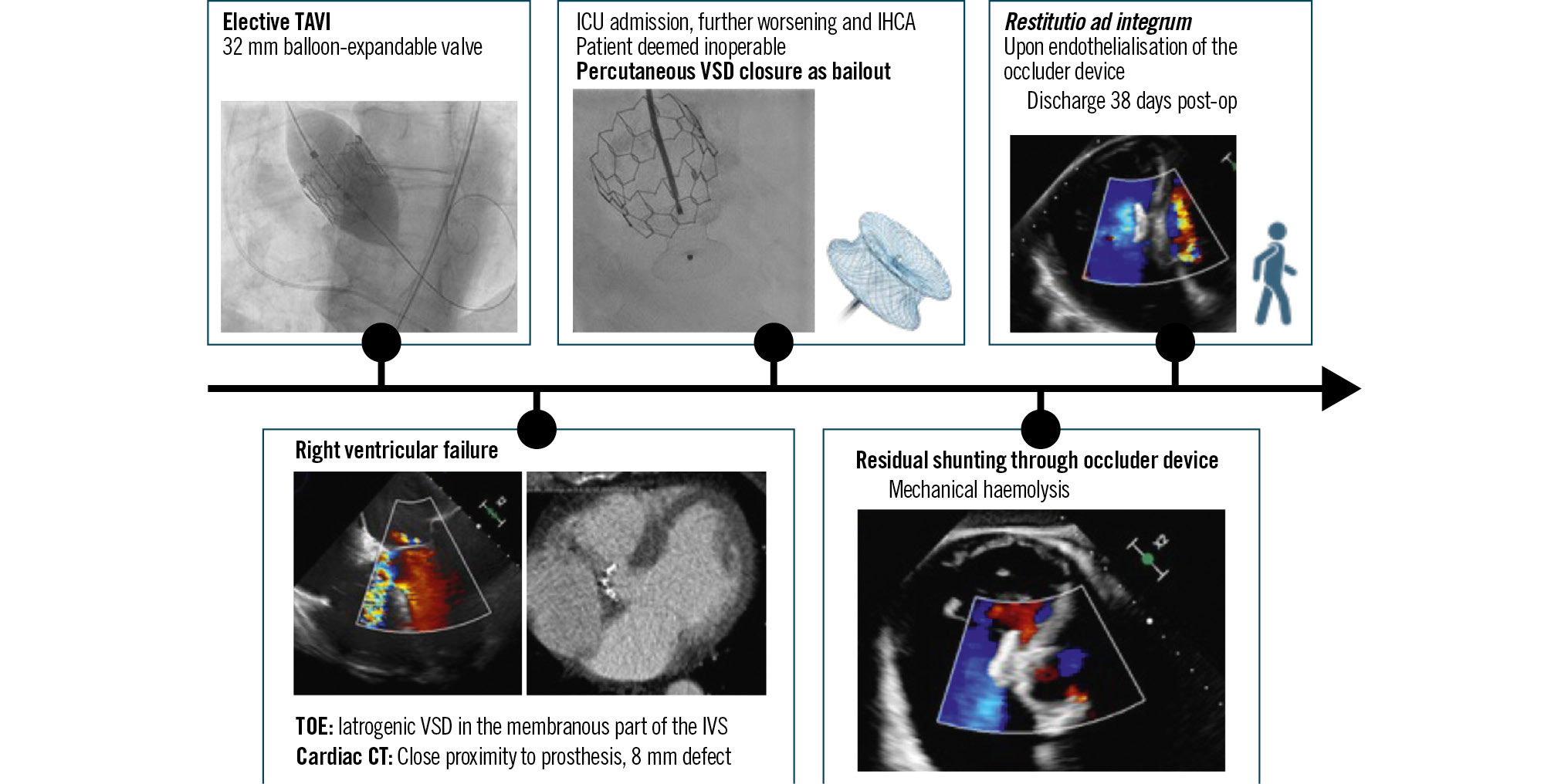
Preoperative diagnostics, including transthoracic echocardiography and cardiac computed tomography (CT), confirmed severe low-flow, low-gradient AS, with a peak transvalvular velocity of 3.6 m/s, a mean gradient of 39 mmHg, and an aortic valve area of 0.4 cm2 (Figure 1A, Figure 1B). Cardiac CT further revealed extensive valvular, subannular, and left ventricular outflow tract (LVOT) calcifications, with a calcium score of 6,476 Agatston units (Figure 1C, Figure 1D).
On the day following admission, the transfemoral implantation of a 32 mm balloon-expandable transcatheter heart valve (Myval Octacor [Meril Life Sciences]) was performed in a standard fashion, resulting in a reduction of the intraprocedural peak-to-peak gradient from 57 mmHg to 2 mmHg. Haemostasis of the puncture site was achieved using a suture-based (Perclose ProStyle [Abbott]) vascular closure device and an additional plug-based (Angio-Seal [Terumo]) vascular closure device. In accordance with institutional standards, the patient was subsequently transferred to the intermediate care unit for further monitoring. Apart from the new onset of a left bundle branch block and transient Mobitz type II second-degree atrioventricular block, the first night after the procedure was uneventful. On physical examination, a holosystolic murmur was noted. Postprocedural echocardiography performed the following day revealed a mild paravalvular leak and an 8 mm iatrogenic VSD located in the membranous portion of the interventricular septum, with a left-to-right shunt (Figure 2A). This finding was confirmed by computed tomography (Figure 2B) and transoesophageal echocardiography (Figure 2C, Figure 2D) plus additional sizing with multiplanar and three-dimensional reconstruction (7x6 mm) (Supplementary Figure 1, Supplementary Figure 2).
In the following days, the patient developed progressive dyspnoea along with hepatic and renal venous congestion as clinical manifestations of right ventricular failure, necessitating admission to the intensive care unit, initiation of non-invasive ventilation, and renal replacement therapy. The patient was deemed inoperable by cardiac surgery due to a high estimated risk of in-hospital mortality (36.1%, according to the European System for Cardiac Operative Risk Evaluation). Conservative management proved unsuccessful, as the patient experienced an in-hospital cardiac arrest due to pulseless ventricular tachycardia. After achieving the return of spontaneous circulation following a brief resuscitation, implantation of a VSD occluder was planned as a bailout therapy.
For VSD occluder implantation (Figure 3), femoral venous and arterial accesses were obtained. From the arterial side, the aortic valve prosthesis was crossed atraumatically using a pigtail catheter (IMPULSE [Boston Scientific]). The VSD was then crossed with a hydrophilic guidewire (GLIDEWIRE [Terumo]) via a Judkins Right 4 catheter (IMPULSE Femoral Right 4 [Boston Scientific]) under transoesophageal echocardiographic guidance. Subsequently, a SAFARI² XS guidewire (Boston Scientific) was positioned in the right ventricular apex via a pigtail catheter. Haemodynamic assessment was performed, followed by defect sizing using a 10×40 mm balloon (Mustang [Boston Scientific]). Finally, the delivery system was advanced, and a 10 mm Amplatzer Muscular VSD Occluder (Abbott) was successfully deployed using a retrograde technique.
The main postprocedural clinical issue was a residual left-to-right minimal shunt through the occluder device (Figure 4), resulting in mechanical haemolysis. An initial increase in lactate dehydrogenase and a decrease in haptoglobin (consistent with haemolysis) were observed; however, these parameters gradually normalised with endothelialisation of the occluder device, as illustrated in Figure 5. No relevant bleeding occurred. As right ventricular function progressively improved, renal replacement therapy was successfully discontinued. Notably, bilirubin levels decreased in parallel, indicating hepatic decongestion (Figure 5). Fifteen days after occluder implantation, the patient was discharged from the intensive care unit, and 23 days later, he was transferred to a rehabilitation centre (Visual Summary).
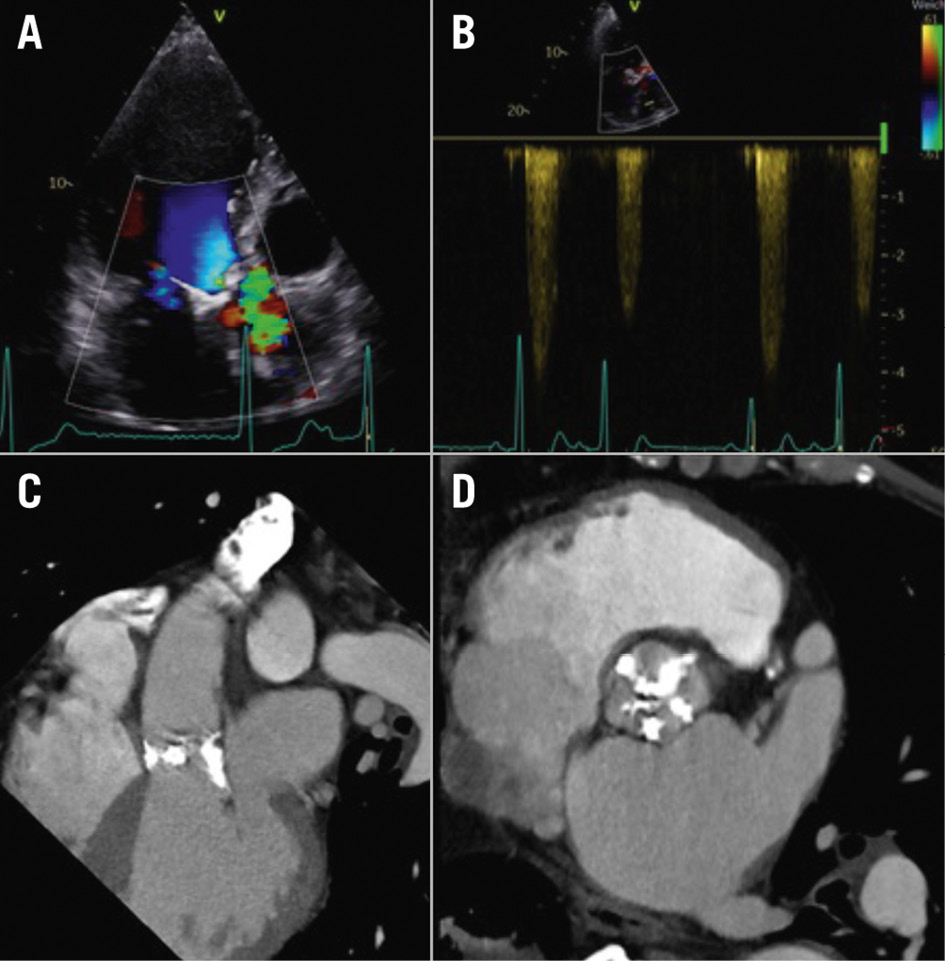
Figure 1. Preoperative diagnostics. A) Transthoracic echocardiogram in the apical three-chamber view with colour Doppler on the aortic valve. B) Transthoracic echocardiogram in the apical three-chamber view with continuous wave Doppler showing a peak transvalvular velocity of 3.6 m/s. C, D) Preoperative cardiac computed tomography showing severe valvular, subannular, and left ventricular outflow tract calcifications with a calcium score of 6,476 Agatston units, confirming a diagnosis of severe aortic stenosis.
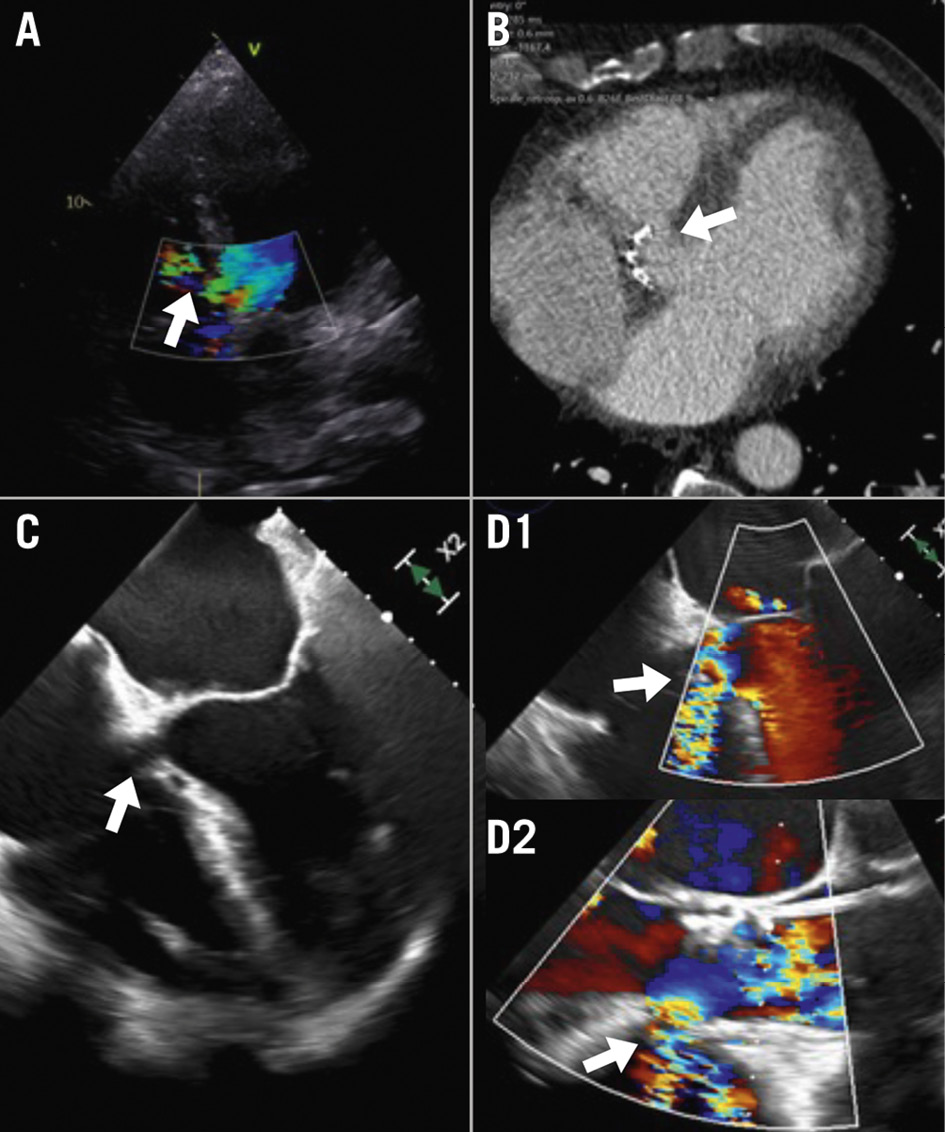
Figure 2. Diagnosis and evaluation of VSD. A) Transthoracic echocardiogram in the apical five-chamber view with colour Doppler on the aortic valve, demonstrating the VSD in the membranous septum. B) Cardiac computed tomography confirming the VSD and enabling precise measurement of the defect. C) Transoesophageal echocardiogram in the mid-oesophageal four-chamber view with a clearly visible defect. D) Transoesophageal echocardiogram in the mid-oesophageal four-chamber view (0°) (D1) with colour Doppler revealing the left-to-right shunt, and the mid-oesophageal three-chamber view (120°) (D2) showing the same shunt. The VSD is indicated by a white arrow in each image. VSD: ventricular septal defect
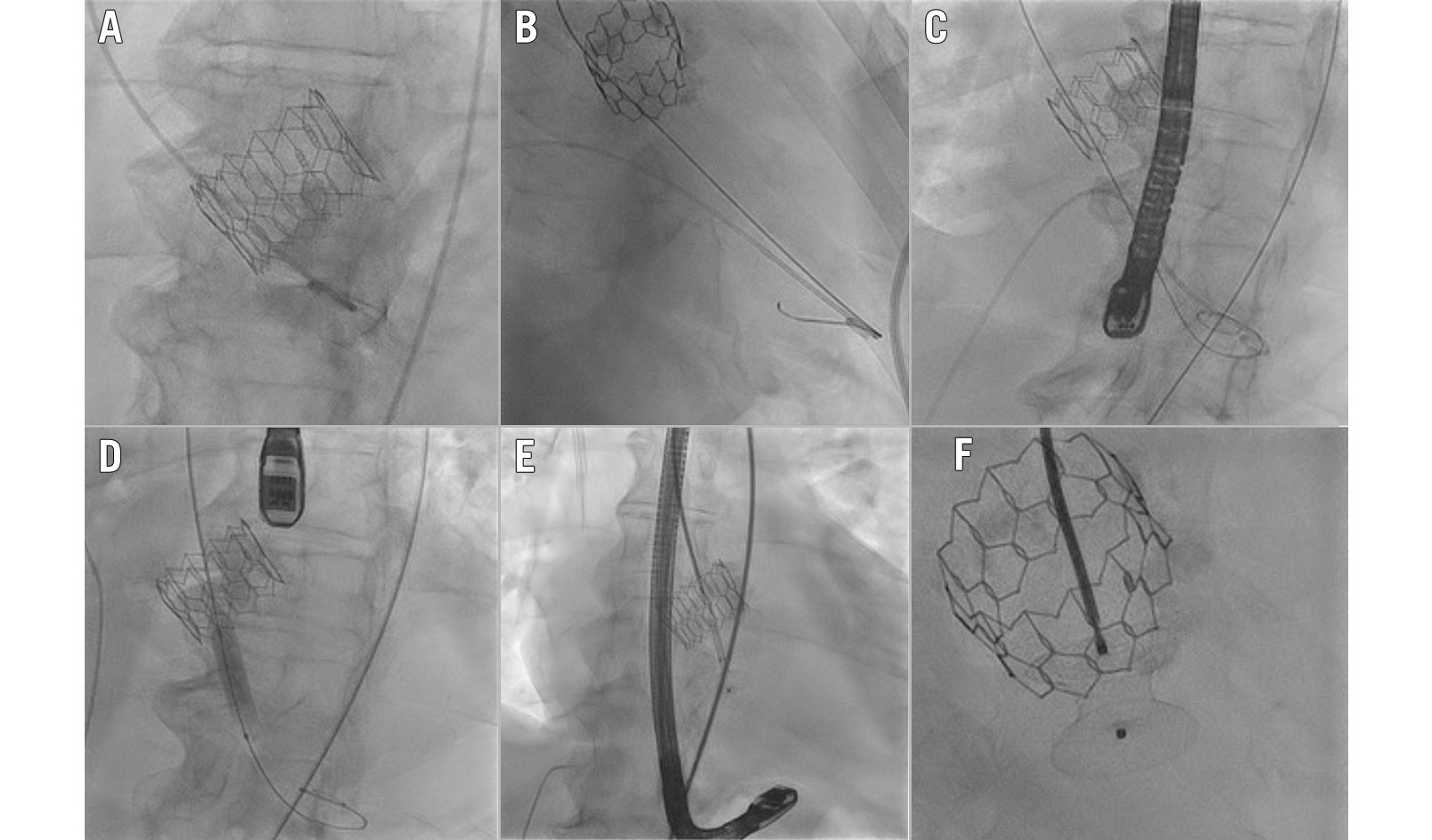
Figure 3. Percutaneous VSD closure using an Amplatzer Muscular VSD Occluder, as seen on fluoroscopic views. A) Passage of the aortic valve prosthesis with a pigtail catheter (IMPULSE). B) The pigtail catheter in the right ventricle and the JR4 catheter (IMPULSE FR4) in the left ventricle. Transoesophageal echocardiography was subsequently used to pass the VSD. C) The SAFARI² XS guidewire is positioned retrogradely in the right ventricular apex via the VSD. The JR4 catheter has already been removed. The pigtail is in the RV via venous femoral access. D) Defect sizing with a 10×40 mm Mustang balloon. E) Deployment of a 10 mm Amplatzer Muscular VSD Occluder via the delivery system from femoral arterial access. F) The pull-and-plug test. RV: right ventricle; VSD: ventricular septal defect
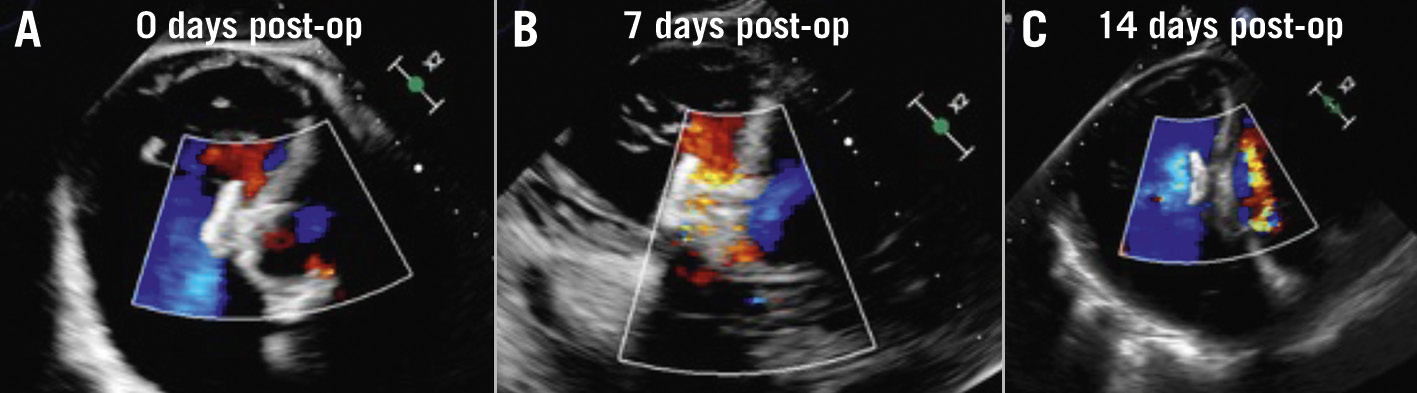
Figure 4. Residual left-to-right shunting through the occluder device, resulting in mechanical haemolysis. Consecutive visualisation of the VSD occluder/membranous part of the intraventricular septum with a transgastric short-axis view in transoesophageal echocardiography. A) An examination from the ICU admission after the procedure, followed by follow-up examinations one week (B) and two weeks (C) later. Note the reduction in the left-to-right shunt upon endothelialisation of the device. ICU: intensive care unit; VSD: ventricular septal defect
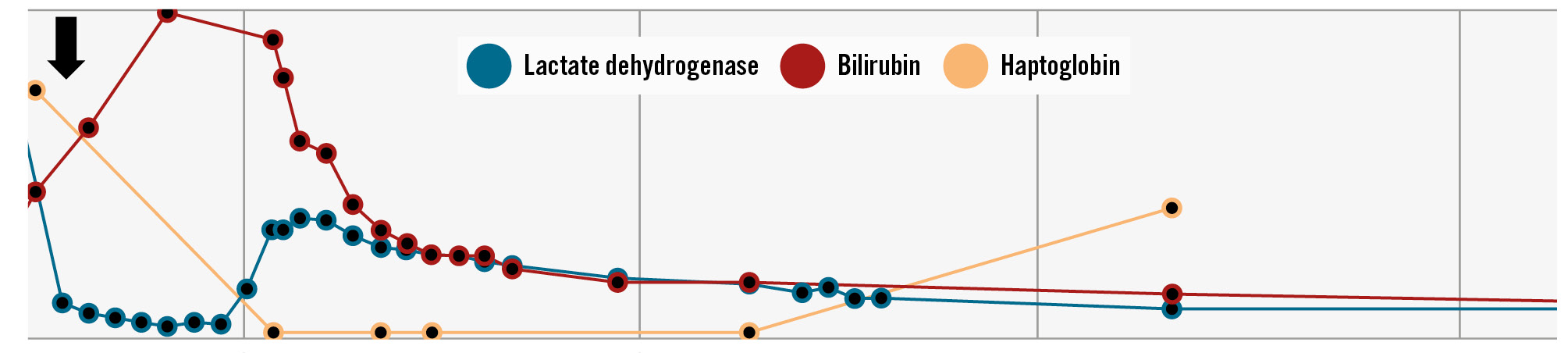
Figure 5. The evolution of haemolysis parameters after the procedure. There is an initial rise in lactate dehydrogenase and a fall in haptoglobin as haemolysis occurs, with normalisation upon endothelialisation of the occluder device. Note the decrease in bilirubin as a sign of liver decongestion. The arrow indicates the time of procedure.
Discussion
Several risk factors for iatrogenic VSD have been proposed, among which the use of balloon-expandable valves (BEV) appears to be particularly significant: more than 80% of reported VSD have occurred, as in the presented case, following implantation of this type of valve.123 Secondly, one of the proposed mechanisms of iatrogenic VSD is mechanical trauma due to annular or subannular calcified nodules; therefore, both the extent and localisation of calcification play an important role in predicting the risk of VSD occurrence.1 We recognise that, in cases of severe LVOT calcification, the evidence suggests that self-expanding valves (SEV) should be preferred to BEV, primarily due to the significantly lower risk of annular rupture. However, both valve types have specific trade-offs. The decisive factor behind the selection of a BEV in the presented case was the extremely large annulus (33 mm in diameter), which exceeded the upper limit of the Evolut (Medtronic) sizing range. The only SEV that could have been used would have been the 35 mm Navitor Titan (Abbott), which was unavailable at the time. Conversely, asymmetric calcium distribution particularly impacts the success of self-expanding valves, carrying a high risk of paravalvular regurgitation.
Most VSD are detected either immediately or within the first week after TAVI, particularly when they present with rapid clinical deterioration and symptoms of heart failure.3 However, the variability in the timing of presentation highlights the importance of maintaining clinical vigilance for this complication in both the immediate postprocedural period and the following weeks.5 Management depends on the clinical presentation and the haemodynamic significance of the defect. Although conservative management may be appropriate in asymptomatic patients with small shunts and minimal haemodynamic impact,8 close monitoring is essential, as untreated symptomatic or haemodynamically significant VSD are associated with poor prognosis and high mortality. In a systematic review by Rojas et al, the 30-day mortality of untreated, symptomatic VSD after TAVI was 35%.1 This is well illustrated in our case, in which the patient required organ support therapy and subsequently suffered a cardiac arrest. These findings underscore the importance of timely intervention, including bailout strategies or approaches with a bridge to definitive treatment.
Percutaneous closure is the preferred treatment for symptomatic patients. Technical challenges include the close proximity to the prosthetic valve and the potential risk of device interference with valve function.12 The Amplatzer Muscular VSD Occluder is the most commonly chosen device in cases of iatrogenic post-TAVI VSD and has been successfully used in multiple cases.1 Alternative devices include the Amplatzer Cribriform Septal Occluder (Abbott)9 and MReye Flipper Detachable Embolization Coil Delivery System (Cook Medical).10 Both antegrade and retrograde strategies of implantation have been reported.2 As there is no dedicated device for the transcatheter closure of membranous VSD, vascular plugs can be used as an alternative. These have been successfully used in many cases of congenital membranous VSD in both children and adults.111213 However, the Amplatzer and MVP (Medtronic) vascular plug systems are primarily intended for arterial and venous embolisation in the peripheral vasculature and are used off-label for closing abnormal shunts or patent ductus arteriosus in selected cases.14 In our opinion, the configuration of the vascular plug has an unfavourable rim/disc-to-waist ratio for the intended use (iatrogenic VSD). The plug has only a 2 mm rim overhang relative to the waist and is oval in shape. This makes it less suitable for use in a membranous septal defect, as it can dislodge very easily. The large disc of a muscular VSD occluder provides a wider seal than the aforementioned vascular plugs and is therefore more suitable for this purpose. The choice of Amplatzer or Occlutech as the system provider should be based on the operator’s expertise and preference.
Although surgical repair seems to be an adequate treatment for iatrogenic VSD, these patients are often poor surgical candidates due to their initial indication for TAVI. Previous case reports have described the successful surgical management of TAVI prosthesis removal, direct suture closure of the defect, reinforced with bovine pericardium and subsequent biological valve implantation,7 as well as VSD patch closure with the TAVI prosthesis left in situ.6
Conclusions
Iatrogenic VSD after TAVI is a rare but serious complication. It might lead to a significant left-to-right shunt and right ventricular failure. Management depends on the VSD size and haemodynamic impact and should be patient-tailored. Early intervention is needed in cases of haemodynamically relevant and symptomatic shunts, as this can prevent malignant deterioration. Percutaneous transcatheter closure is feasible as a bailout in inoperable patients but may lead to further complications, i.e., mechanical haemolysis.
Impact on daily practice
The presence of symptoms of right ventricular failure after TAVI should raise the suspicion of VSD. Timely intervention is essential for symptomatic iatrogenic VSD.
Consent statement
Consent was obtained from the patient for publication of this case report.
Conflict of interest statement
E. Tigges received honoraria and/or consulting fees and/or grants from Edwards Lifesciences, Medtronic, Abbott, Philips, Boston Scientific, AstraZeneca, J&J Medtech, Shockwave Medical, and Resuscitec - all not related to the present work; and reports participation on advisory board for Edwards Lifesciences, Medtronic, Abbott, and Shockwave Medical. T. Ubben received support for attending meetings from Abbott and Boston Scientific - all not related to the present work. D.-U. Chung received consulting fees from Medtronic; and honoraria from Philips - all not related to the present work. The other authors have no conflicts of interest to declare.