Device position and coronary angiographic findings: (A,B) sequential deployment of the left ventricular and right ventricular discs with stable septal apposition. C,D) Left ventricular angiography confirming satisfactory device position before and after device release. E) Coronary angiography showing mid-left anterior descending artery total occlusion. F) Coronary angiography showing distal right coronary artery disease. VT: ventricular tachycardia
Learning objectives
- Post-infarction ventricular septal rupture should be suspected in patients presenting late after myocardial infarction with abrupt haemodynamic deterioration.
- Transcatheter closure may offer a life-saving alternative in patients unsuitable for surgical repair.
- Apical ventricular septal rupture with friable, dissected septal tissue requires meticulous procedural planning, careful device selection, and a stable delivery strategy.
Ventricular septal rupture (VSR) is an uncommon but catastrophic mechanical complication of acute myocardial infarction and remains associated with very high mortality despite contemporary reperfusion strategies.12 Clinical deterioration is often abrupt, particularly in patients presenting late with cardiogenic shock, pulmonary oedema, and electrical instability.2 Although urgent surgical repair remains the standard treatment, outcomes are frequently limited in critically ill patients by friable infarcted tissue, technical complexity, and evolving multiorgan dysfunction.34 In this setting, transcatheter closure has emerged as a pragmatic alternative in selected patients, offering the immediate reduction of left-to-right shunting and rapid haemodynamic stabilisation.56
While transcatheter closure of post-infarction VSR is well documented in the literature, with numerous case reports, retrospective studies, and registries describing this approach as an alternative to surgery, the present case contributes several distinct clinical and procedural insights. The intervention was performed as an emergency salvage procedure in a patient with profound cardiogenic shock, recurrent ventricular tachycardia, and worsening multiorgan failure – without mechanical circulatory support and without any delay for tissue maturation, as any such delay would likely have been fatal. We report successful closure using a simplified transjugular approach allowing direct right-to-left ventricular crossing without arteriovenous loop formation, guided primarily by transthoracic echocardiography, with an intentionally oversized septal occluder to ensure stable anchoring in friable infarcted tissue.
Case summary
A 64-year-old male presented with a 48-hour history of severe chest pain followed by sudden-onset dyspnoea and syncope. On arrival, he was in profound cardiogenic shock with a blood pressure of 80/56 mmHg and a heart rate of 132 beats/min, accompanied by acute pulmonary oedema. His course was further complicated by multiple episodes of haemodynamically unstable ventricular tachycardia requiring direct current (DC) cardioversion, intravenous amiodarone, and transient cardiopulmonary resuscitation.
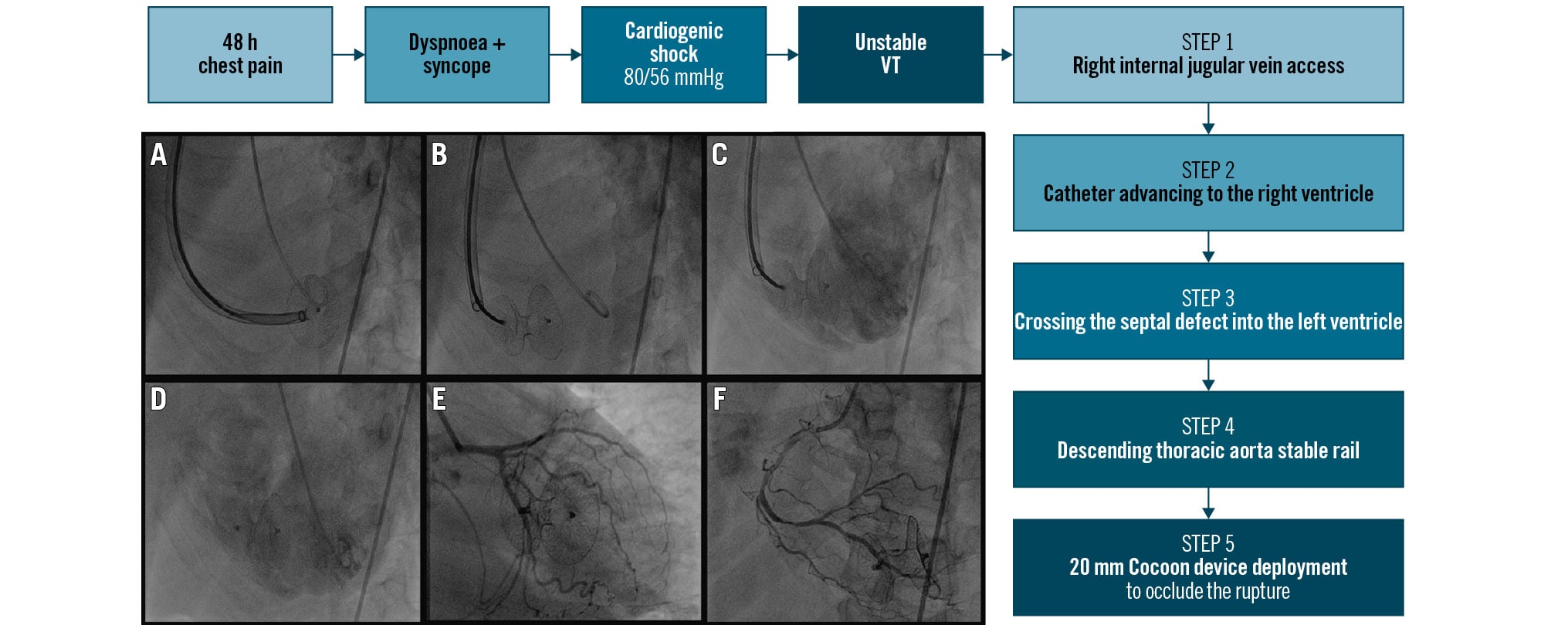
A clinical examination revealed elevated jugular venous pressure, bilateral basal crepitations, a third heart sound, and a loud pansystolic murmur, raising suspicion of a post-infarction mechanical complication. Electrocardiography demonstrated sinus tachycardia with pathological Q waves and persistent ST-segment elevation in leads V1-V6, consistent with late-presenting anterior ST-segment elevation myocardial infarction (Figure 1).
Transthoracic echocardiography demonstrated an akinetic aneurysmal anterior wall and distal interventricular septum with a large apical ventricular septal rupture measuring 10×12 mm. The septal tissue appeared friable, with intraseptal dissection and multiple right ventricular exit sites, resulting in a significant left-to-right shunt (ratio of pulmonary to systemic blood flow [Qp/Qs] 2.9:1) (Figure 1, Moving image 1). Additional findings included severe mitral regurgitation, moderate tricuspid regurgitation, and a left ventricular ejection fraction of 40-45%.
Laboratory testing demonstrated a marked systemic inflammatory response and evolving multiorgan dysfunction, including leucocytosis (24,600/μL; neutrophils 91%), elevated procalcitonin (3 ng/mL) and C-reactive protein (112 mg/L) levels, thrombocytopaenia (94×10⁹/L), renal dysfunction (serum creatinine 2.4 mg/dL; blood urea 98 mg/dL), hyperbilirubinaemia (1.9 mg/dL), and marked transaminitis (aspartate aminotransferase/alanine aminotransferase ratio 1267/823 U/L). An arterial blood gas analysis showed metabolic acidosis with a lactate level of 2.7 mmol/L.
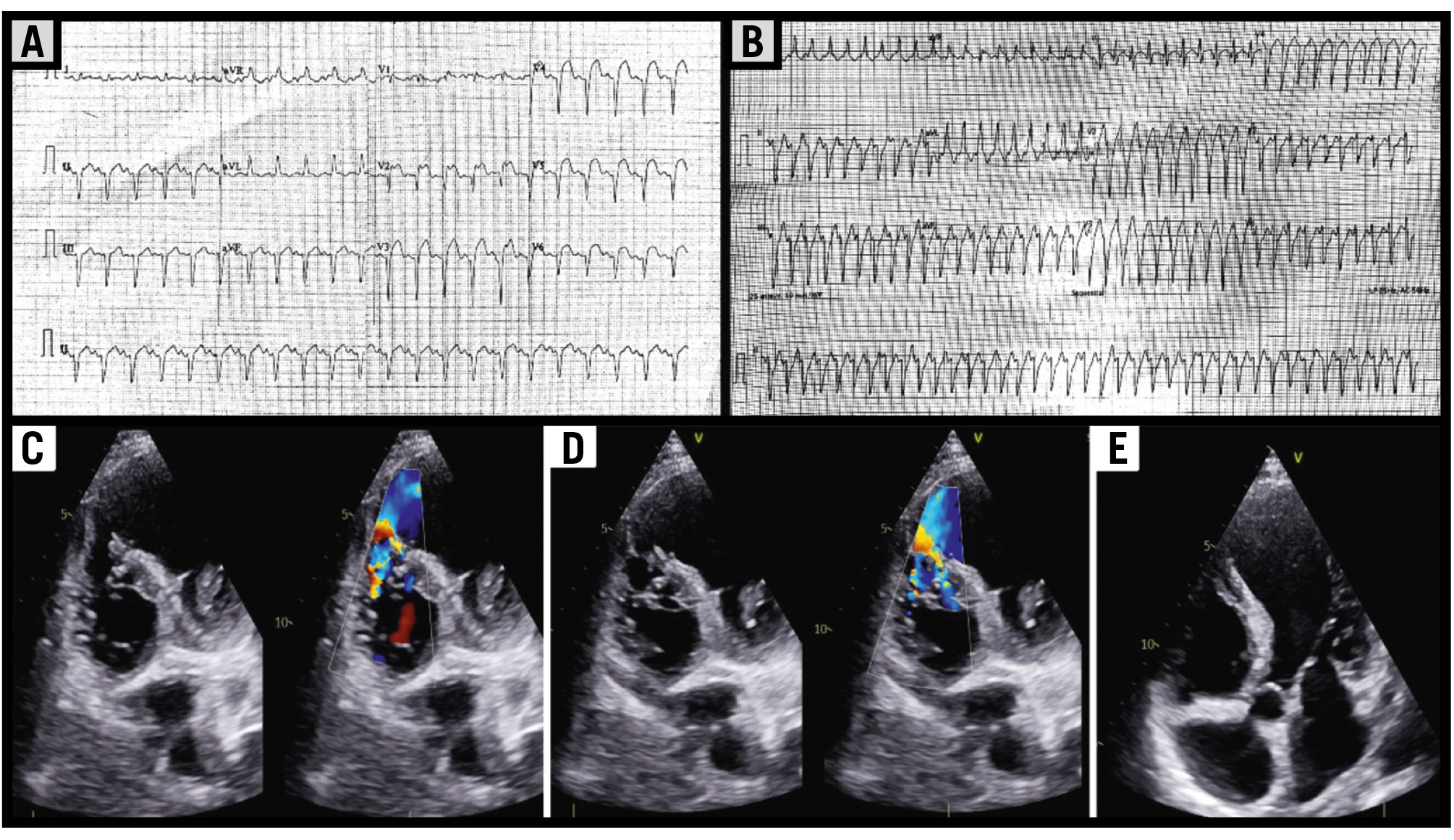
Figure 1. Electrocardiographic and echocardiographic findings at presentation. A) Baseline ECG showing anterior ST-segment elevation myocardial infarction. B) Repeat ECG showing sustained monomorphic ventricular tachycardia during haemodynamic deterioration. C,D) Transthoracic echocardiography with colour Doppler demonstrating a large apical ventricular septal rupture with left-to-right shunting. E) Echocardiographic image showing the apical ventricular septal defect with intraseptal dissection. ECG: electrocardiography
Management strategy
The patient was managed with non-invasive ventilatory support, vasopressors, intravenous loop diuretics, continuous amiodarone infusion, and broad-spectrum antibiotics. Readiness for escalation to invasive mechanical ventilation and intra-aortic balloon pump (IABP) support was maintained because of ongoing haemodynamic instability. An IABP was not ultimately inserted; given the lack of consistent evidence of a mortality benefit with an IABP in cardiogenic shock and economic considerations, the decision was made to proceed without mechanical circulatory support. However, an IABP was kept on standby for immediate use in the event of further haemodynamic deterioration.
Mechanical circulatory support options were carefully evaluated prior to intervention. Neither venoarterial extracorporeal membrane oxygenation nor Impella (Abiomed) were utilised because of unavailability and economic constraints. Preprocedurally, haemodynamic optimisation was achieved with vasopressor support, non-invasive ventilation, and intravenous loop diuretics to reduce preload. Pharmacological afterload reduction with vasodilators was avoided at this stage because of the systemic hypotension and large left-to-right shunt, as vasodilation in this context risked precipitating cardiovascular collapse. Following successful device closure and haemodynamic stabilisation, vasopressors were gradually weaned and discontinued. Afterload reduction was subsequently initiated with intravenous nitroglycerine and low-dose angiotensin-converting enzyme inhibitors, which are beneficial in the post-closure phase to reduce left ventricular wall stress and support myocardial recovery.
The patient presented approximately 48 hours after the onset of chest pain with syncope secondary to recurrent ventricular tachycardia, requiring transient cardiopulmonary resuscitation and DC cardioversion. Immediate medical management was initiated, including vasopressor support and non-invasive ventilation. Following urgent transthoracic echocardiographic assessment and biochemical evaluation confirming a large VSR with significant shunting and evolving multiorgan dysfunction, a decision to proceed with transcatheter closure was made on the same day, without delay for haemodynamic stabilisation, as further deterioration was anticipated. The procedure was performed emergently on the day of presentation. Post-intervention, the patient demonstrated rapid haemodynamic and clinical improvement, allowing the gradual reduction and subsequent discontinuation of vasopressors. With stabilisation, afterload reduction was initiated using intravenous nitroglycerine.
The current approach to managing a post-infarction VSR typically involves delaying intervention for 2 to 6 weeks. This delay allows for the maturation of the infarct and fibrotic stabilisation, which are linked to improved procedural outcomes. However, in our patient, there was ongoing cardiogenic shock, a significant left-to-right shunt (Qp/Qs of 2.9), and worsening multiorgan dysfunction, which made it impossible to stabilise the haemodynamics and rendered a delayed repair unfeasible. As a result, we opted for urgent transcatheter closure as a salvage strategy. While early intervention has been associated with higher mortality rates, this association is inconsistently reported and likely influenced by selection bias. Patients who present with severe shock and electrical instability are inherently at a higher risk for early mortality and often do not survive long enough for a delayed repair.7
This case posed a major therapeutic dilemma regarding both timing and mode of intervention. The patient had presented late after anterior myocardial infarction with cardiogenic shock, recurrent ventricular arrhythmias, and evolving multiorgan dysfunction, all features associated with extremely high mortality.128 Although urgent surgical repair is conventionally recommended, the combination of haemodynamic instability, friable necrotic septal tissue, and end-organ dysfunction rendered surgery prohibitively high risk.34 Following a multidisciplinary Heart Team discussion, emergency transcatheter closure was selected as a salvage strategy.
Transcatheter closure
The procedure was performed under fluoroscopic and transthoracic echocardiographic guidance. Procedural guidance was primarily achieved using transthoracic echocardiography in conjunction with fluoroscopy. Left ventricular angiography was performed in a limited manner and only for essential anatomical delineation. A comprehensive transthoracic echocardiographic assessment provided adequate structural detail; therefore, transoesophageal echocardiography was deferred in view of the haemodynamic instability and the need for a rapid, less invasive approach. Multislice computed tomography was avoided because of underlying renal dysfunction and the necessity to minimise contrast exposure. Intracardiac echocardiography was not utilised due to lack of availability at our centre.
Vascular access was obtained via the right femoral artery (7 Fr) and right internal jugular vein (7 Fr). Left ventriculography in a steep left anterior oblique cranial projection delineated a large aneurysmal apical septal cavity with a ventricular septal rupture measuring up to 12 mm and significant left-to-right shunting (Figure 2, Moving image 2).
Given the apical location of the rupture, the defect was intentionally crossed from the right ventricular side using a 0.035 inch curved-tip hydrophilic guidewire supported by a Judkins right diagnostic catheter (Moving image 3). The wire was advanced across the rupture into the left ventricle and then into the descending thoracic aorta. The catheter was advanced over the wire, after which the hydrophilic wire was exchanged for an extra-stiff 0.035 inch Amplatz exchange length guidewire (Boston Scientific), which was positioned securely in the descending aorta.
This direct transjugular right-to-left ventricular crossing strategy created a stable rail for device delivery while avoiding the need for a conventional arteriovenous loop, thereby simplifying the procedure in this haemodynamically unstable patient. Over the extra-stiff wire, a 10 Fr delivery sheath was advanced across the defect into the left ventricular cavity.
A 20 mm Cocoon Septal Occluder (Vascular Innovations/Sahajanand Medical Technologies) was selected despite the maximal defect diameter of 12 mm to provide stable anchoring in the setting of friable infarcted tissue, intraseptal dissection, and multiple right ventricular exit sites. Defect sizing was performed using transthoracic echocardiography in conjunction with limited left ventriculography, with careful minimisation of contrast use. The largest measured diameter across both modalities (10-12 mm) was used to guide device selection. In line with established practice for post-infarction VSR, intentional oversizing in the range of approximately 1.5-2 times the measured defect diameter was applied to ensure stable anchoring in the friable, dissected septal tissue. Device selection was further guided by the specific technical characteristics of the Cocoon Septal Occluder and operator experience with its use in post-infarction VSR. The device provides a relatively large left ventricular disc, which is advantageous in this setting, facilitating effective sealing and stability across necrotic and dissected tissue. Its double-disc design and radial strength support secure anchoring across friable septal margins, and it has been used in reported series of post-myocardial infarction VSR closure.910 The apical location provided adequate landing zones without significant risk of interference with the mitral valve or chordae.
The device was advanced through the delivery sheath and deployed under fluoroscopic and echocardiographic guidance. The left ventricular disc was opened within the left ventricular cavity and positioned before deployment of the right ventricular disc (Moving image 4, Moving image 5). Final imaging demonstrated satisfactory device position, stable seating across the rupture, and a marked reduction in residual shunting (Moving image 6). Following reassessment of device position, residual shunt, and surrounding structures, the device was released (Visual Summary, Moving image 7). The final procedural result was confirmed using multimodality assessment. Transthoracic echocardiography demonstrated appropriate device position, stable seating, and a significant reduction in left-to-right shunting (Qp/Qs <1.5), along with reassessment of ventricular function and exclusion of pericardial effusion or valvular compromise. These findings were supported by angiographic assessment and concurrent haemodynamic improvement.
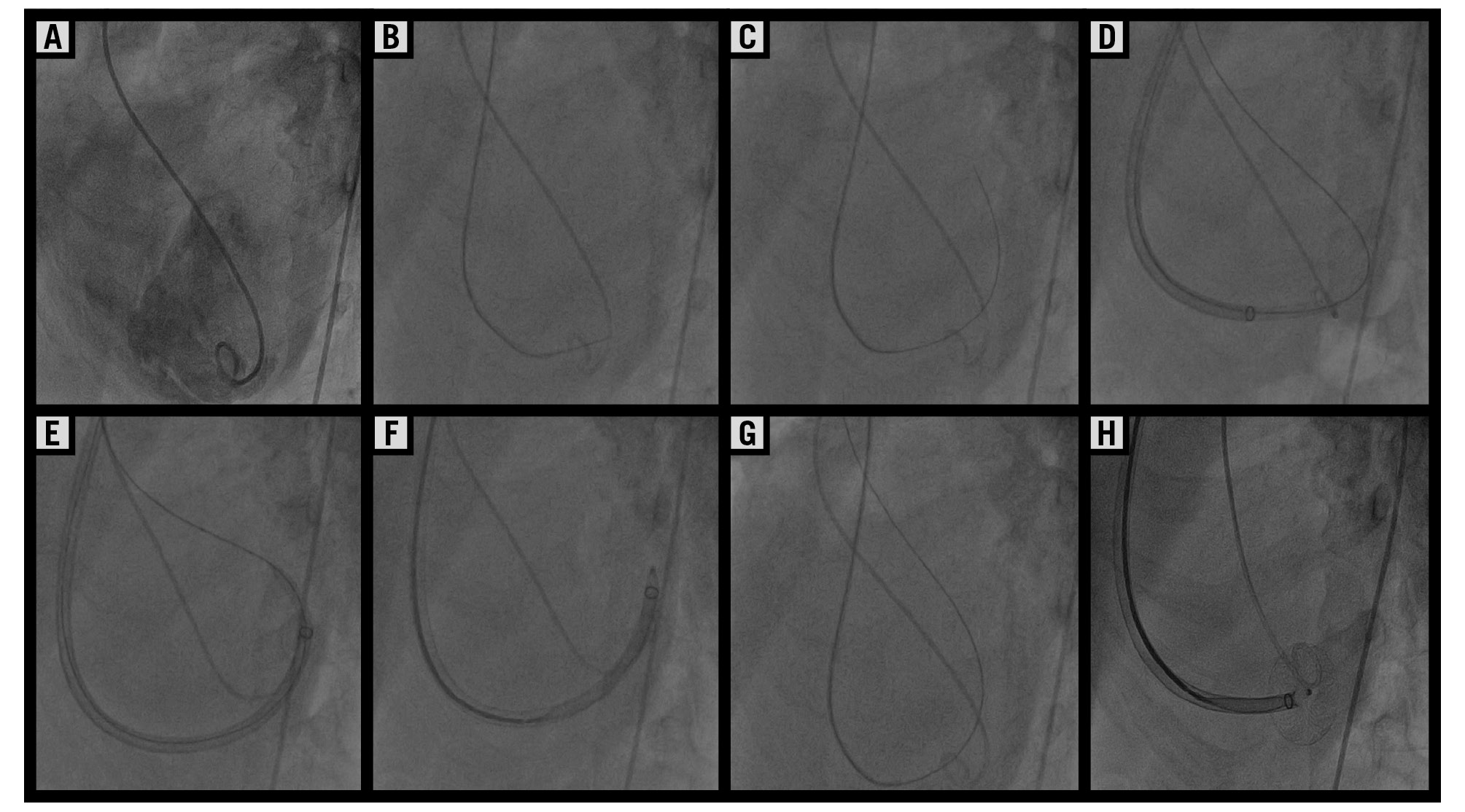
Figure 2. Transcatheter closure of the apical post-infarction ventricular septal rupture. A) Left ventricular angiography in the LAO cranial projection demonstrating a large apical ventricular septal rupture with left-to-right shunting and adequate margins. B,C) A 0.035 inch hydrophilic curved-tip wire was advanced across the defect from the right ventricle to the left ventricle using a Judkins right diagnostic catheter. D) The wire was advanced into the descending aorta, creating a stable rail. E,F) An atrial septal sheath was advanced across the defect into the left ventricular cavity. G,H) The septal occluder was positioned across the defect, with opening of the left ventricular disc in the left ventricular cavity. LAO: left anterior oblique
Clinical outcome
Following transcatheter closure, the patient demonstrated early haemodynamic improvement, with a progressive reduction in vasopressor requirements and no recurrence of sustained ventricular tachycardia. Respiratory status improved with continued supportive care, and serial echocardiography confirmed a stable device position with only trivial residual left-to-right shunting. This was accompanied by gradual recovery of end-organ function. The patient was discharged in a stable condition 4 days after the procedure. At 6-month follow-up, the patient remained clinically well, with sustained haemodynamic and functional improvement. Echocardiography demonstrated a reduction of mitral regurgitation to mild-to-moderate severity and recovery of left ventricular systolic function, with an estimated ejection fraction of ~50%. A small residual left-to-right shunt was seen across the device, without evidence of device displacement, residual instability, or haemolysis (Figure 3, Moving image 8).
Following clinical recovery, a myocardial perfusion scan demonstrated non-viable myocardium in the left anterior descending artery (LAD) territory with inducible ischaemia in the right coronary artery (RCA) territory. Subsequent coronary angiography confirmed mid-LAD total occlusion and distal RCA disease. Given the absence of viable myocardium in the LAD territory, revascularisation of the occluded LAD was not pursued. Percutaneous coronary intervention to the RCA was successfully performed for the inducible ischaemia identified in that territory.
Regarding arrhythmia management, the patient initially presented with recurrent haemodynamically unstable ventricular tachycardia, managed with DC cardioversion and intravenous amiodarone. Following successful defect closure and haemodynamic stabilisation, no further episodes of sustained ventricular tachycardia were observed during the index hospitalisation or at 6-month follow-up. The patient was discharged on guideline-directed medical therapy including beta blockers and oral amiodarone. Implantable cardioverter-defibrillator implantation was recommended at follow-up; however, it was deferred because of financial constraints, with a plan for reassessment at subsequent review.
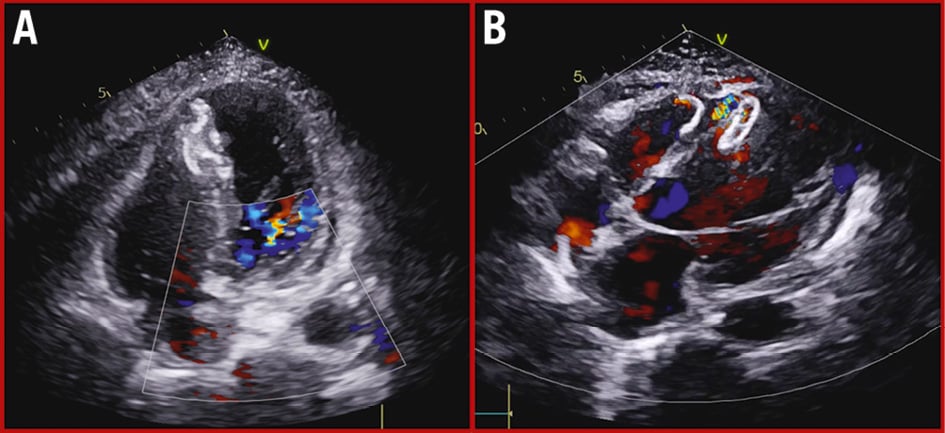
Figure 3. Transthoracic echocardiography at 6 months. At 6-month follow-up, transthoracic echocardiography demonstrated a stable device position on the four-chamber view. A) A modified four-chamber view (B) revealed a minimal residual left-to-right shunt across the device.
Discussion
Post-infarction ventricular septal rupture remains associated with extremely high mortality, particularly in patients presenting with cardiogenic shock.12 Although urgent surgical repair remains the conventional treatment, operative mortality is substantial in the acute phase, especially in haemodynamically unstable patients with friable infarcted myocardium.34
In this context, transcatheter closure has emerged as a pragmatic rescue strategy in patients with prohibitive surgical risk. Registry data and observational studies have demonstrated acceptable procedural success and survival in selected anatomically suitable patients, although outcomes remain strongly dependent on haemodynamic status.56 Cardiogenic shock remains the most important predictor of mortality, underscoring the importance of rapid haemodynamic stabilisation.28 Although the transcatheter closure of post-infarction VSR is not a novel concept, the present case highlights the feasibility of a streamlined, time-efficient strategy – achieved without mechanical circulatory support, without arteriovenous loop formation, and without delaying intervention for tissue maturation – in one of the most haemodynamically compromised clinical presentations described in the literature.
The present case highlights several important technical considerations. The apical location of the rupture poses inherent challenges due to the unfavourable angulation and limited septal support, which may compromise device alignment when conventional femoral venous access is used.11 Although left-sided access with arteriovenous loop formation is commonly described in the literature, it was intentionally avoided in this case. Given the apical location and haemodynamic instability, the right internal jugular venous approach provided a more direct, coaxial trajectory, enabling controlled and rapid device delivery. Avoidance of arteriovenous loop formation further reduced procedural complexity and duration, which is of particular importance in critically unstable patients. In addition, the transjugular approach represents our default institutional strategy, with which operators are familiar, facilitating efficient catheter manipulation in the catheterisation laboratory.
Procedural simplification was a key strategic priority. Conventional techniques often rely on arteriovenous loop formation to enhance support during device delivery, but such manoeuvres may increase procedural duration and haemodynamic instability in critically ill patients. In the present case, intentional right-to-left ventricular crossing with advancement of the guidewire into the descending aorta created a stable rail without loop formation, thereby reducing the technical complexity while maintaining adequate support.
Device selection in post-infarction VSR differs fundamentally from that in congenital defects because the target substrate consists of necrotic, friable, and often dissected tissue. Prior studies have emphasised the importance of device oversizing to ensure stable anchoring and minimise residual shunting.910 Residual shunts are common and should be interpreted in the context of haemodynamic improvement rather than complete angiographic closure. Potential risks associated with device oversizing in this setting include device embolisation from inadequate tissue support, valvular interference from oversized discs, and erosion of adjacent structures; however, the apical location – remote from the atrioventricular valves and basal conduction system – provided a favourable landing zone that minimised these risks.
The timing of intervention remains a major clinical challenge and one of the most debated aspects of post-infarction VSR management. Contemporary literature and expert consensus favour a strategy of haemodynamic stabilisation followed by delayed definitive repair in the fibrotic phase, typically 2 to 6 weeks after myocardial infarction.12 During this period, progressive fibrosis of the necrotic septal margins reduces tissue friability, improves anchoring conditions for both surgical and transcatheter repair, and is associated with meaningfully lower procedural mortality compared with emergency intervention on acutely necrotic tissue.910 Mechanical circulatory support – most commonly the intra-aortic balloon pump – plays a central role in this strategy, reducing left ventricular afterload, decreasing the left-to-right shunt fraction, and providing haemodynamic stabilisation as a bridge to definitive repair.13 In the present case, persistent cardiogenic shock, a large left-to-right shunt (Qp/Qs 2.9), recurrent haemodynamically unstable ventricular tachycardia, and rapidly worsening multiorgan dysfunction precluded any meaningful stabilisation, rendering delayed intervention unfeasible. Early transcatheter closure was therefore undertaken as a salvage strategy driven entirely by clinical necessity. As detailed in the management strategy, the ‘stabilise and delay’ approach was not applicable in this patient, and the decision for emergency transcatheter closure was made on the basis of clinical necessity rather than as a general preference for early intervention.7
This case supports the expanding role of transcatheter closure as a lifesaving option in selected high-risk patients with post-infarction VSR. It also highlights that a direct transjugular antegrade strategy may offer procedural advantages in apical VSR by improving alignment, reducing technical complexity, and enabling rapid device delivery in haemodynamically unstable patients.
Conclusions
Emergency transcatheter closure may provide effective haemodynamic rescue in selected patients with post-infarction apical ventricular septal rupture and prohibitive surgical risk. In anatomically challenging apical defects, a direct transjugular strategy may improve procedural feasibility and facilitate controlled device delivery.
Impact on daily practice
Transcatheter closure can be life-saving in selected patients with post-infarction ventricular septal rupture who are unsuitable for surgery. In haemodynamically unstable patients, procedural simplification is critical. A direct transjugular right-to-left ventricular crossing strategy with a stable aortic rail may facilitate device delivery while avoiding conventional arteriovenous loop formation. This case highlights the importance of early recognition, careful procedural planning, and individualised intervention in this lethal mechanical complication of myocardial infarction.
Consent statement
Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
Conflict of interest statement
The authors have no conflicts of interest to declare.