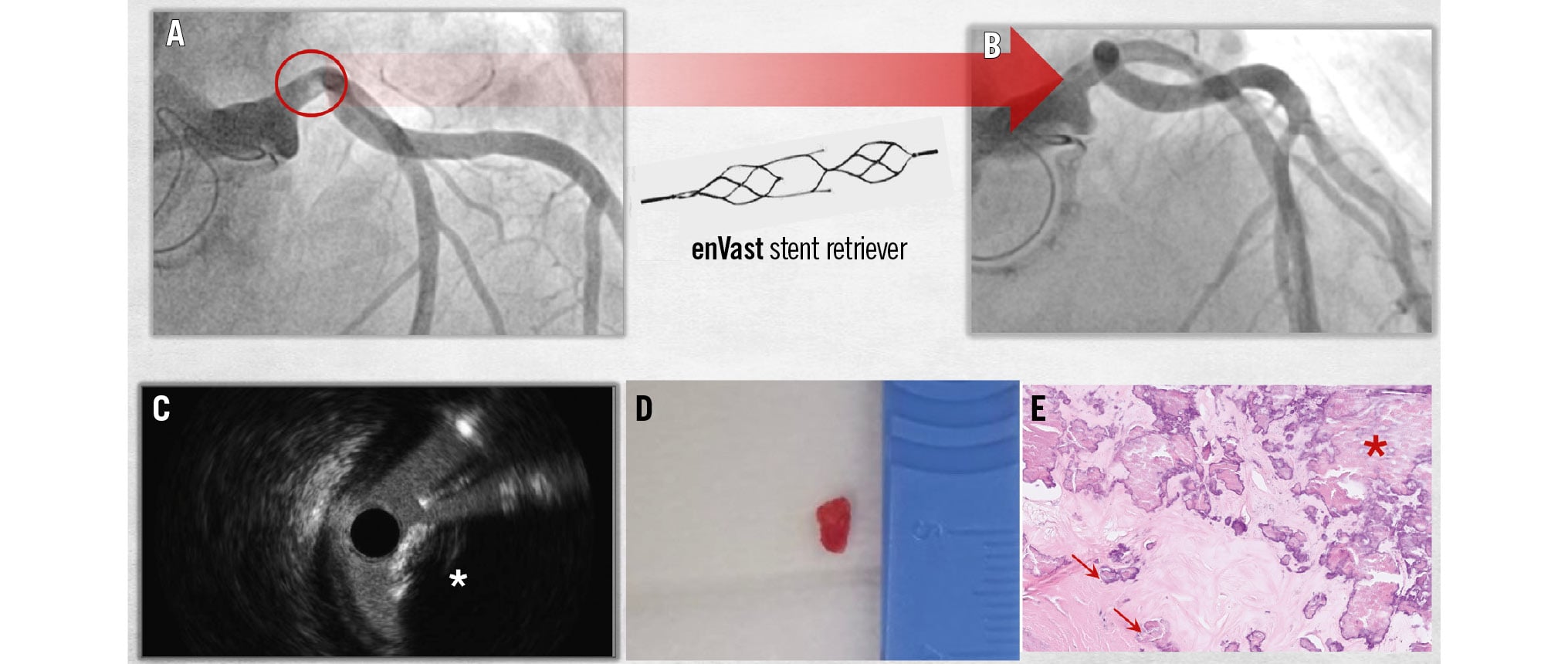
A) Postoperative coronary angiogram showing a new radiolucent structure in the distal left main coronary artery (circle). B) Post-extraction angiogram showing successful embolus removal using the enVast stent retriever. C-E) Multidimensional depiction of the embolic material: (C) intravascular ultrasound showing a calcified nodular structure; (D) macroscopic aspect after extraction; (E) histopathological analysis showing coarse (asterisk) and fine calcifications (arrows) interspersed with connective and adipose tissue, supporting its origin from the native aortic valve.
Learning objectives
- To understand the mechanisms and causes of coronary obstruction following aortic valve replacement
- To develop a differential diagnosis algorithm based on the timing of presentation, angiographic findings (both preoperative and postoperative), and intravascular imaging
- To recognise the role of advanced thrombectomy devices in the extraction of non-thrombotic emboli, as well as their potential complications
Coronary artery obstruction after surgical aortic valve replacement (SAVR) is a rare but well-documented complication. It most commonly arises from coronary embolisation of valve tissue or thrombus or from direct intraoperative injury. The use of advanced thrombectomy devices, such as the enVast (Vesalio) stent retriever, has become essential in managing high thrombotic burden, especially when traditional aspiration methods fall short. Here, we present a unique case involving the successful retrieval of a calcified embolus using the enVast stent retriever following SAVR, highlighting the device’s potential role in managing such complications (Visual Summary).
Case summary
A 75-year-old female with a history of hypertension presented to our institution with symptomatic severe aortic valve stenosis. A preoperative coronary angiography revealed only minor wall irregularities. After a Heart Team discussion, the patient underwent a minimally invasive transaxillary SAVR with a 23 mm Perimount Magna Ease bioprosthesis (Edwards Lifesciences). The immediate postoperative transoesophageal echocardiography showed good function of the aortic prosthetic valve, though a stunned left ventricle was also noted, prompting the initiation of a milrinone infusion. Over the following hours, a dynamic rise in cardiac biomarkers was observed (high-sensitivity troponin [hs-Tn] 8,472 ng/L, upper limit of normal [ULN] <14 ng/L; creatine kinase myocardial band [CK-MB] 343 μg/L, ULN <4.7 μg/L), accompanied by episodes of non-sustained ventricular tachycardia. Given the clinical presentation consistent with postoperative non-ST-segment elevation myocardial infarction, the catheterisation laboratory team was called for urgent coronary angiography.
Six French (6 Fr) right femoral access was obtained, and coronary angiography revealed minor wall irregularities in the right coronary artery. However, a round, radiolucent lesion was noted in the distal left main coronary artery (LMCA) (Figure 1A, Moving image 1), which was not visible on the preoperative angiogram. An intravascular ultrasound (IVUS) pullback from the left anterior descending artery (LAD) to the LMCA revealed a protruding structure with a hyperechoic surface and posterior acoustic shadowing (Figure 1B, Moving image 2), consistent with calcific material. Adjacent fibrous plaque was also observed, without evidence of plaque rupture or thrombus. Given these findings, a calcified embolus was suspected, and we proceeded with an attempt at extraction using an enVast stent retriever (4.5×37 mm) (Figure 2A). Following the first extraction attempt, distal migration of the embolus to the mid-LAD occurred, resulting in impaired distal flow (Figure 2B, Moving image 3). After the second attempt (Figure 2C), we successfully captured and removed the calcified material from the LAD. However, due to its size, the embolus, contained within the enVast device, could not pass through the guiding catheter and became lodged just outside its tip. Consequently, we performed en bloc retrieval of the entire system, which included the enVast device, the guiding catheter, and the femoral sheath. This was done after securing the femoral access by advancing a highly supportive coronary guidewire, which enabled the placement of a new femoral sheath. After coronary re-engagement and a new angiogram, we confirmed complete removal of the foreign material and restoration of Thrombolysis in Myocardial Infarction (TIMI) 3 flow, although a dissection in the mid- and distal LAD became evident (Figure 2D, Moving image 4). We decided to treat it with 2.5×40 mm and 3.5×40 mm Essential PRO drug-eluting balloons (iVascular) (Figure 2E, Figure 2F). The angiographic result was excellent, with preserved TIMI 3 flow (Figure 2G, Figure 2H and Moving image 5, Moving image 6). The patient experienced a gradual recovery during the postoperative period and was ultimately discharged in stable condition.
The extracted material measured approximately 5×3×3 mm (Figure 3A) and had a spherical to triangular shape with a pale red colour and a distinctly firm consistency on palpation, suggestive of calcified tissue. Histological evaluation revealed granular calcifications interspersed with connective and adipose tissue, supporting its origin from the native aortic valve (Figure 3B1, Figure 3B2). Additionally, a small fragment of vascular wall was identified (Figure 3C).
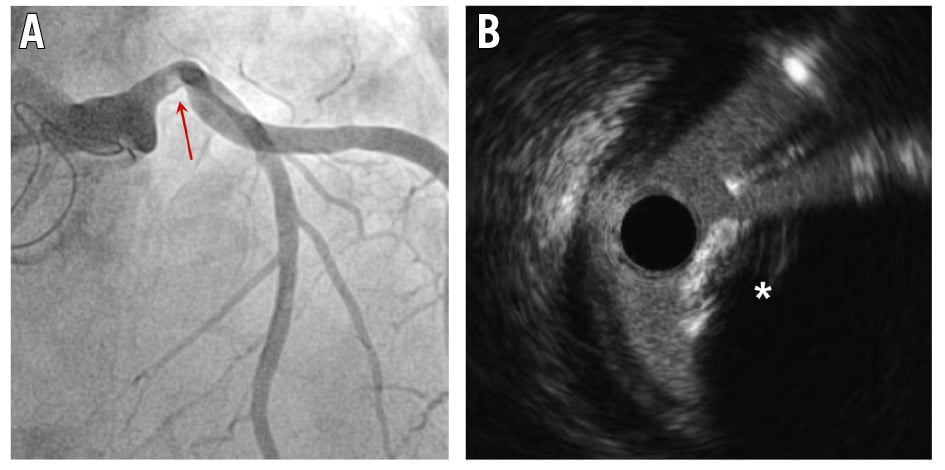
Figure 1. Postoperative coronary angiogram and IVUS. A) Coronary angiogram showing a spherical, radiolucent lesion in the distal left main coronary artery (LMCA; red arrow). B) Intravascular ultrasound (IVUS) pullback from the left anterior descending artery to the LMCA, revealing a protruding lesion (asterisk) with a hyperechoic surface and acoustic shadowing, consistent with a calcified embolus.
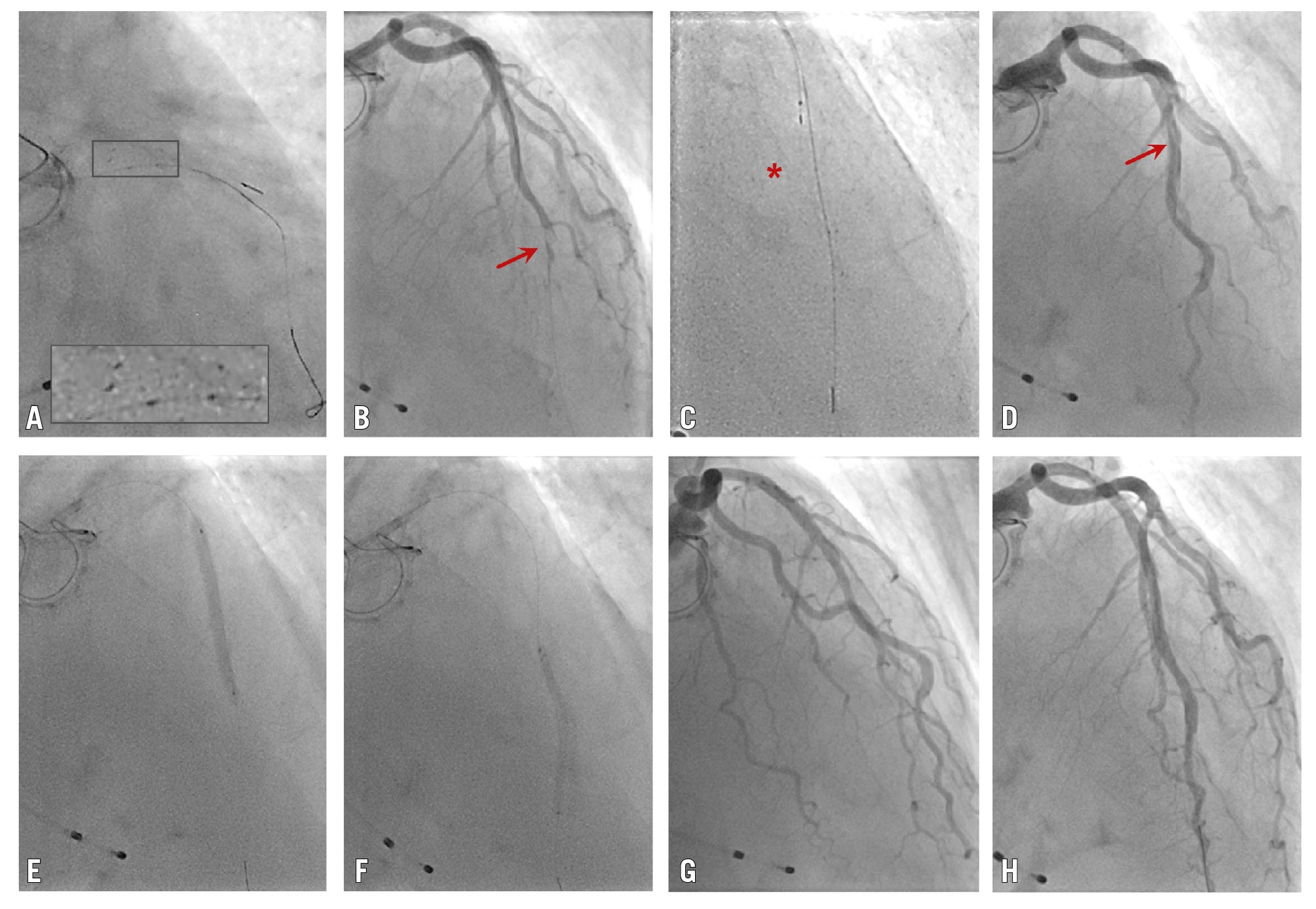
Figure 2. Embolic extraction using the enVast stent retriever. A) The enVast stent retriever (4.5×37 mm) is deployed in the distal left main and proximal left anterior descending artery (LAD). A magnified view of the boxed region (inset) highlights the four radiopaque points corresponding to the device’s “dropping zones”. B) Distal migration of the embolus up to the mid-LAD (red arrow) after the first extraction attempt, resulting in impaired distal flow. C) Second extraction attempt with the device placed at the mid-LAD (red asterisk). D) Post-extraction angiogram showing successful embolus removal and restoration of flow, although a dissection flap is evident at the mid-LAD (red arrow). E, F) Percutaneous coronary intervention of the mid- and distal LAD using drug-eluting balloons. G, H) Final angiogram showing minor dissections and TIMI 3 flow. TIMI: Thrombolysis in Myocardial Infarction
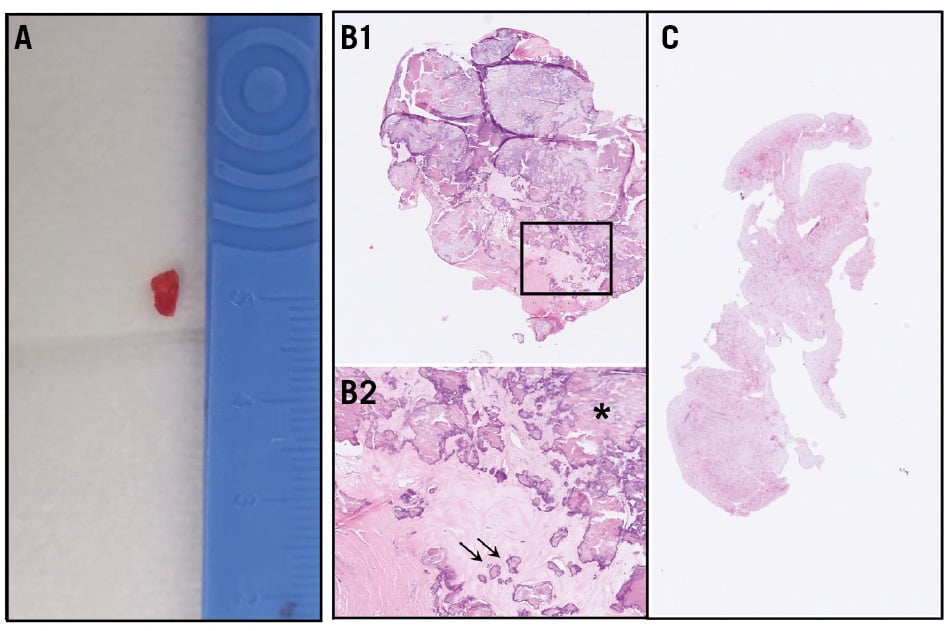
Figure 3. Analysis of extracted embolic material. A) Extracted embolus, macroscopic aspect.B1) Histopathological analysis of the extracted embolus (haematoxylin and eosin stain, 5× digital magnification). B2) Magnified view of the boxed region in B1 showing fibrous stroma with coarse (asterisk) and fine calcifications (arrows; haematoxylin and eosin stain, 20× digital magnification). C) Fragments of vascular wall (haematoxylin and eosin stain, 1.6× digital magnification).
Discussion
Coronary obstruction following SAVR is an uncommon but recognised complication, with a reported incidence of approximately 0.7-0.9% at 12 months, and is slightly more frequent than after transcatheter aortic valve implantation (TAVI), where the reported incidence ranges from 0.2-0.4% at 12 months.12
Several mechanisms may account for coronary events after SAVR. In the acute setting, three main mechanisms are typically considered.3 The first is coronary embolisation, which may involve calcified debris originating from disrupted plaques in the native aortic valve, the coronary arterial walls, or the manipulated aorta; thrombus formed at cannulation sites and embolised to the coronaries through retrograde perfusion; or air bubbles. The second mechanism is direct coronary injury related to intraoperative manipulation, including ostial obstruction due to prosthesis malposition or excessive tightening of the aortic valve suture ring, ostial thrombosis secondary to trauma caused by the aortic retractor, or coronary artery dissection.4 The third potential mechanism is coronary artery spasm triggered by intraoperative catecholamine release. Conversely, in the subacute period, typically within 3-6 months after surgery, coronary ostial obstruction is thought to result from progressive intimal fibrous thickening, which may be caused by turbulent blood flow in the aortic root induced by a prosthetic valve.5 Also, in the subacute period and in the late phase after aortic valve replacement, prosthetic valve thrombosis with coronary embolism should be suspected, especially in the setting of mechanical valve replacement.6 Finally, and regardless of the timing, an acute coronary event related to a pre-existing atherosclerotic plaque should always be considered in the differential diagnosis.
In our case, the spherical, radiolucent angiographic appearance of the lesion was compatible with either a thrombotic or calcific aetiology. Intravascular ultrasound (IVUS) demonstrated a protruding lesion with a hyperechoic surface and acoustic shadowing, suspected to be calcium. Given the baseline angiogram, which demonstrated no pre-existing coronary lesions, calcific embolisation was considered the most likely diagnosis.
We decided to use the enVast stent retriever device in an off-label fashion, which resulted in successful embolic extraction. The enVast device is the first and only European Conformity-approved and U.S. Food and Drug Administration-cleared large thrombus burden retriever to facilitate flow restoration to the coronary circulation.78 It consists of a self-expanding nitinol stent that is advanced through a microcatheter, featuring large open pockets – known as “dropping zones” − which serve as entry points for capturing thrombi. The risk of embolisation to side branches or the peripheral circulation during device retrieval is particularly pronounced when the thrombus is located distally in the vessel. In such cases, a guide extension catheter may be positioned proximally to the stent retriever. As the stent retriever is retracted into the guide extension, simultaneous vacuum-assisted aspiration is performed using one to three vacuum syringes connected to the Y-connector of the guiding catheter.7 In our case, given the initial proximal location of the embolus, the use of a guide extension catheter would not have provided additional safety against embolisation into the peripheral circulation. Additionally, it would have further reduced the effective inner lumen of the aspiration system, adding extra difficulty to our attempt to retrieve a bulky and calcified embolus. The use of this device has been previously reported as an effective off-label strategy for the management of calcified embolic material after TAVI.910 To the best of our knowledge, this is the first report describing the use of the enVast device for the retrieval of calcified embolic material following SAVR.
Despite the procedural success, the use of this device was not without complications, including initial distal migration of embolic material and vessel dissection during a subsequent, more distal attempt. In fact, histopathological analysis of the extracted material revealed a portion of the vessel wall alongside the calcified embolus, suggesting intimal damage caused by the device. It can be hypothesised that both complications are more likely to occur during off-label use of the enVast device, particularly when the extracted material is calcific rather than thrombotic. A hard, calcified embolus may be more prone to distal migration compared with a softer thrombus, which can be more easily captured by the device. Also, vessel dissection may be attributed to the nature of the calcific material; specifically, calcific spikes may protrude through the stent struts, tearing the vessel wall as the device is retracted proximally. Notably, no instances of vessel dissection have been reported following use of the enVast device.78 Overall, these findings emphasise the need for caution and careful consideration when employing this device for off-label indications.
Several alternatives are available for retrieving calcified embolic material from the coronary arteries. Conventional manual aspiration catheters are limited by vacuum strength and small lumen diameters, making them potentially ineffective for retrieving calcified emboli. The mother-and-child technique, which uses a larger guiding catheter (up to 7 Fr or 8 Fr) with a smaller catheter or guide extension inside, facilitates direct aspiration. In our case, however, even an 8 Fr system would not have provided a large enough lumen for safely extracting an embolus with a maximum diameter of 5 mm. Furthermore, it may not have eliminated the need for en bloc extraction of the entire system, relying solely on the negative pressure from manual vacuum to prevent material detachment and embolisation as the system is withdrawn rather than benefiting from the additional safety provided by the metallic mesh of the enVast device. Among advanced thrombectomy devices, the Indigo System CAT RX catheter (Penumbra) offers high vacuum power and has been used in post-TAVI cases,10 although the extracted emboli were smaller. Although the alternatives mentioned may have reduced the likelihood of success in our case, they could potentially minimise vessel wall trauma, making them worth considering on a case-by-case basis.
Conclusions
This case highlights the successful management of a calcified embolus using the enVast stent retriever after SAVR. The device, initially designed for large thrombus burden retrieval, proved effective in removing calcified embolic material and restoring coronary flow. However, this case also underscores the challenges associated with the off-label use of this device, including the risks of distal embolisation and vessel dissection, which necessitate additional caution and careful management.
Impact on daily practice
The embolisation of calcified tissue can be a cause of coronary obstruction and postoperative acute coronary syndrome after aortic valve replacement. A differential diagnosis includes thrombotic embolism and pre-existing calcific nodules. Intravascular imaging and preoperative angiograms are key to distinguishing these since the management of each differs substantially. Calcified emboli can be successfully extracted with the enVast stent retriever system, although operators must be aware of possible complications (e.g., distal migration, coronary dissection).
Consent statement
The patient gave informed consent for the publication of this case.
Acknowledgements
The authors would like to express their gratitude to Dr L.P. Priesterbach-Ackley for kindly providing the histological images of the extracted embolus.
Funding
No funding was received for the preparation or publication of this manuscript.
Conflict of interest statement
W.K. den Dekker has received consultant fees from Vesalio. J.F. Bulnes received a conference travel grant from Vesalio. D. M. Muijs reports no conflict of interest.