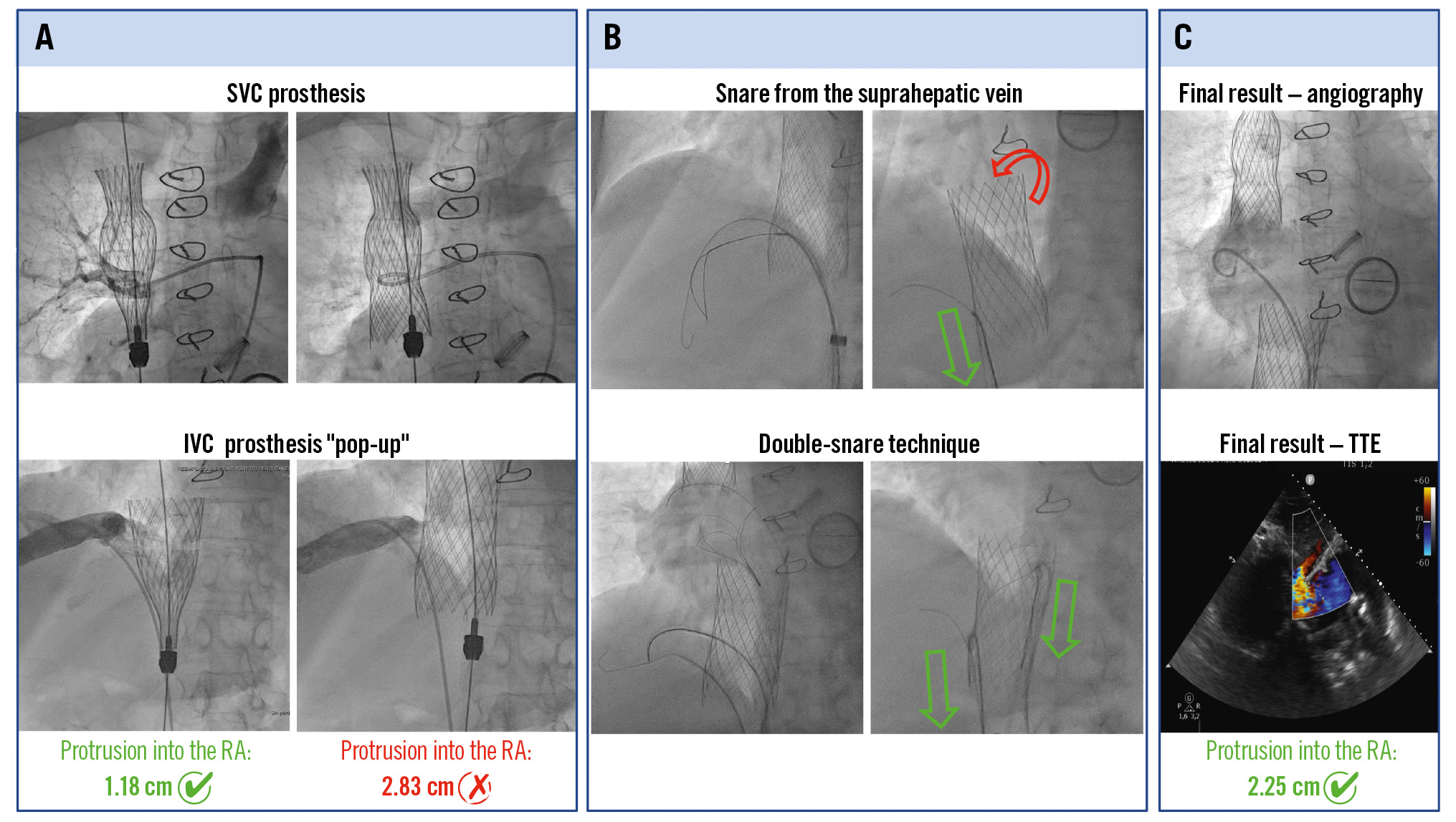
A) Upward migration of the prosthesis. B) The double-snare technique. C) Final result on angiography and TTE. IVC: inferior vena cava; RA: right atrium; SVC: superior vena cava; TTE: transthoracic echocardiography
Learning objectives
- To recognise inferior vena cava prosthesis migration as a potential complication during TricValve system implantation
- To understand the role of snare-based techniques in device retrieval and repositioning
- To highlight the importance of rapid decision-making and technical strategy in managing procedural complications
Severe tricuspid regurgitation (TR) is associated with poor clinical outcomes during follow-up and represents a growing therapeutic challenge.1 Depending on the anatomical characteristics of the tricuspid apparatus, a wide range of transcatheter therapies are currently available. In patients deemed to be at high or prohibitive surgical risk, heterotopic valve replacement has emerged as an alternative treatment strategy.2
Caval valve implantation (CAVI) is a palliative transcatheter approach aimed at reducing systemic venous congestion through the deployment of prosthetic valves in the vena cava. The TricValve system (Products & Features GmbH) was specifically developed for this purpose and has demonstrated promising results in terms of symptom relief and a reduction in heart failure (HF) hospitalisations.34
Although the procedure is relatively straightforward compared with other structural interventions, complications may occur. Among these, prosthesis malpositioning or migration represent particularly challenging scenarios that require prompt recognition and management.23
We report a case of inferior vena cava (IVC) prosthesis migration during TricValve system implantation and its successful percutaneous management using a double-snare technique.
Case presentation
Patient presentation and past medical history
We present the case of a 68-year-old female with massive TR and multiple recurrent hospitalisations due to decompensated HF. As regards her past cardiovascular history, she underwent surgical aortic and mitral valve replacement with mechanical valves due to rheumatic heart disease 20 years earlier and presented with atrial fibrillation on oral anticoagulation. Her comorbidities included chronic obstructive pulmonary disease and obesity (body mass index 34 kg/m²). She was on guideline-directed medical therapy, including bisoprolol, eplerenone, valsartan, and loop diuretics.
At presentation, she reported progressive peripheral oedema, abdominal distension, and reduced functional capacity (New York Heart Association [NYHA] Class III-IV symptoms). Physical examination revealed jugular vein distention and signs of venous congestion.
Diagnosis
Transthoracic echocardiography (TTE) demonstrated preserved left ventricular ejection fraction, with both prosthetic left-sided valves functioning normally. Moreover, it showed massive functional TR (a vena contracta of 14 mm and systolic flow reversal in the hepatic veins) with severe annular dilatation (43 mm), a lack of valvular coaptation, and right ventricular (RV) dysfunction (with a tricuspid annular plane systolic excursion of 18 mm and an RV fractional area change of 28%) (Figure 1). Right heart catheterisation confirmed elevated right-sided pressures and prominent V waves in both the superior and inferior vena cava (22 mmHg), consistent with severe venous congestion. The pulmonary artery pressure was 32/12 mmHg (mean: 24 mmHg). Coronary angiography showed no significant coronary artery disease.
Computed tomography was performed for procedural planning, confirming suitable anatomy for CAVI, with adequate dimensions of the superior and inferior vena cava and preserved distance from the suprahepatic veins (Figure 1).
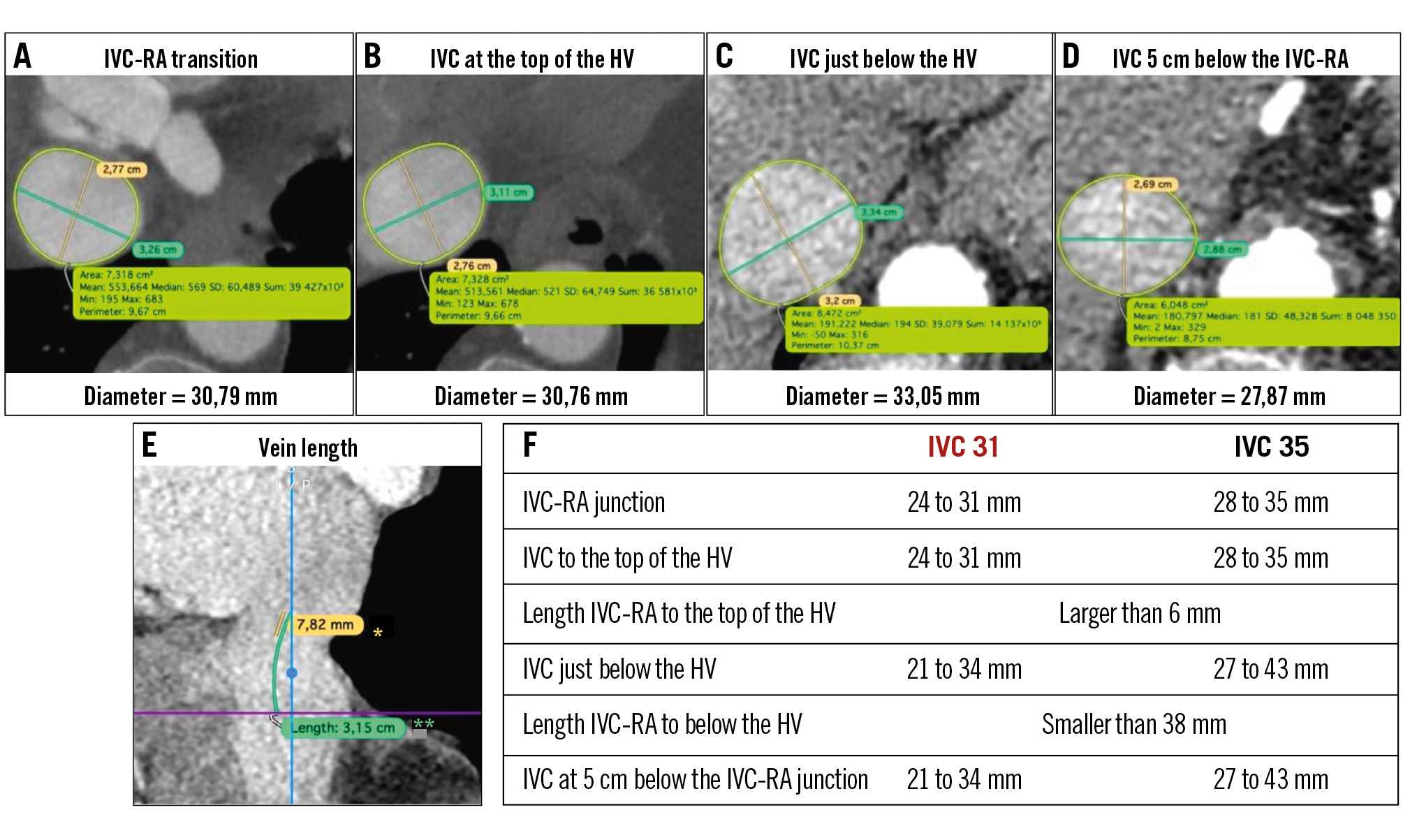
Figure 1. Preprocedural tomography measurements. A-D) Axial cuts at different anatomical reference points of the IVC, showing their respective measurements and diameters. E) The sagittal cut demonstrating IVC length. *Distance from the IVC-RA junction to the top of the hepatic veins; **distance from the IVC-RA junction to just below the hepatic veins. F) Size ranges for the 31 mm and 35 mm IVC prostheses of the TricValve system. Based on these measurements, the 31 mm IVC prosthesis (red) was selected for our patient. HV: hepatic vein; IVC: inferior vena cava; RA: right atrium
Management and procedure
Given her high surgical risk (European System for Cardiac Operative Risk Evaluation (EuroSCORE) II 5.27%), unfavourable anatomy for transcatheter edge-to-edge repair (due to severe annular dilatation and leaflet malcoaptation), and the fact that orthotopic transcatheter tricuspid valve replacement (EVOQUE system [Edwards Lifesciences]) is currently not available in Argentina, the Heart Team recommended treatment with the TricValve system.
The procedure was performed under conscious sedation. Venous access was obtained via the left femoral vein and right femoral vein (5 Fr and 27 Fr delivery systems, respectively).
A 25 mm TricValve system prosthesis was successfully implanted in the superior vena cava (SVC), using the innominate vein and right pulmonary artery as anatomical landmarks (Figure 2).
Subsequently, a 31 mm TricValve system prosthesis was advanced for implantation in the IVC, using the suprahepatic veins as anatomical landmarks and guided by TTE (Figure 3A). During deployment, an unintended upward migration (“pop-up”) of the valve into the right atrium (RA) occurred, resulting in a significant protrusion of 2.83 cm into the RA and significant paravalvular leakage detected on TTE (Figure 3B, Moving image 1).
Initial attempts to reposition the TricValve system prosthesis using a single snare (Amplatz Goose Neck [Medtronic]) from the suprahepatic vein were unsuccessful and resulted primarily in device tilting rather than effective repositioning (Figure 4A, Moving image 2).
Given this limitation, a double-snare strategy was implemented using an Amplatz Goose Neck snare from the suprahepatic vein and an EN Snare (Merit Medical) from the upper crown of the IVC prosthesis.
To deploy the snare from the suprahepatic vein, we used a 7 Fr Judkins right (JR) catheter that was advanced through one of the rhomboid cells of the IVC prosthesis. Subsequently, a 0.035″ J-tip guidewire was advanced through a different rhomboid cell using a 5 Fr JR catheter; this wire was then used for snaring and downward traction from the suprahepatic vein.
Deployment of the EN Snare from the upper crown of the prosthesis was more challenging. A 5 Fr JR catheter was first advanced into the IVC prosthesis, then directed outward through a rhomboid cell into the prosthesis-vein interface and subsequently readvanced into the prosthesis lumen over a 0.035″ J-tip guidewire. A 7 Fr femoral left guide catheter was then advanced through the IVC prosthesis lumen into the RA, allowing for the delivery of the EN Snare to capture the 0.035″ J-tip guidewire in the right atrium (Figure 4B). All the devices were advanced through the right and left femoral vein accesses obtained at the beginning of the procedure.
This technique allowed us to apply traction from different directions, via separate venous accesses, allowing for improved control over prosthesis orientation and movement (Moving image 3). The simultaneous traction enabled gradual and controlled repositioning of the valve towards a more desirable position.
Final angiographic and TTE assessment confirmed a stable and more favourable prosthesis position, with a protrusion into the RA of 2.25 cm (Moving image 4, Moving image 5). Despite not achieving the intended landing zone (RA protrusion <15 mm),5 this final position resulted in the complete abolition of paravalvular leakage. The suprahepatic veins remained patent, and no further procedural complications were observed (Figure 4C).
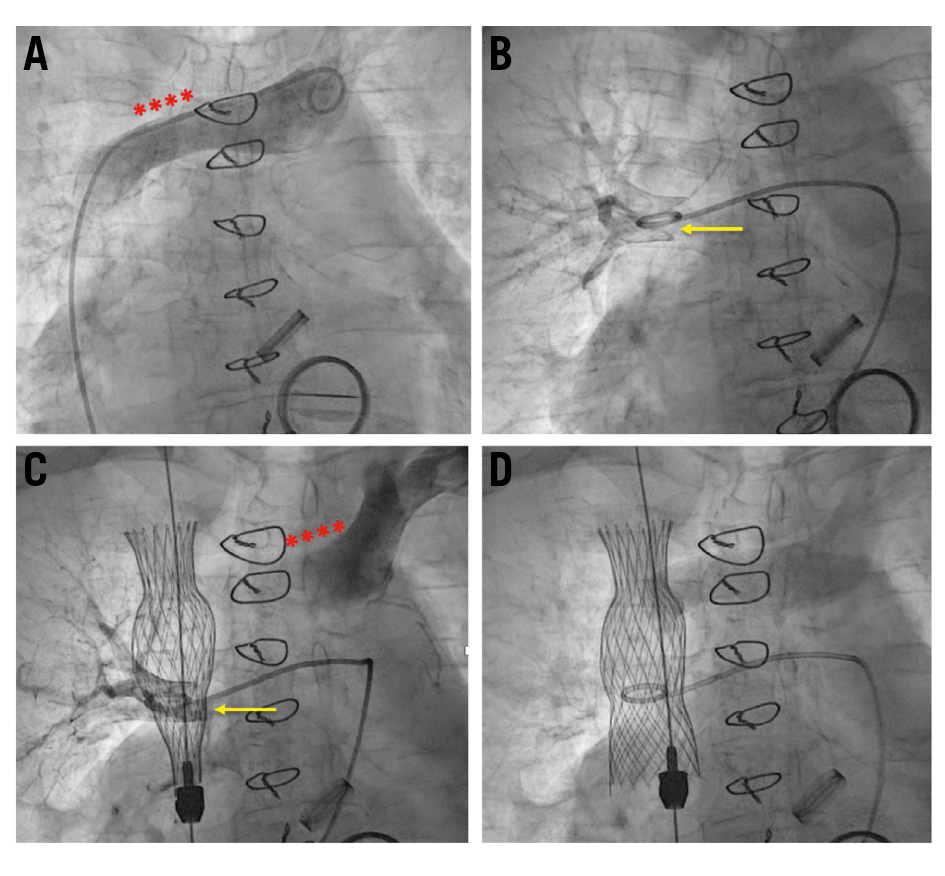
Figure 2. Superior vena cava TricValve system prosthesis implantation. A) Anatomical landmark (red asterisks): innominate vein; (B) anatomical landmark (yellow arrow): right pulmonary artery; (C, D) implantation of 25 mm superior vena cava prosthesis TricValve system.
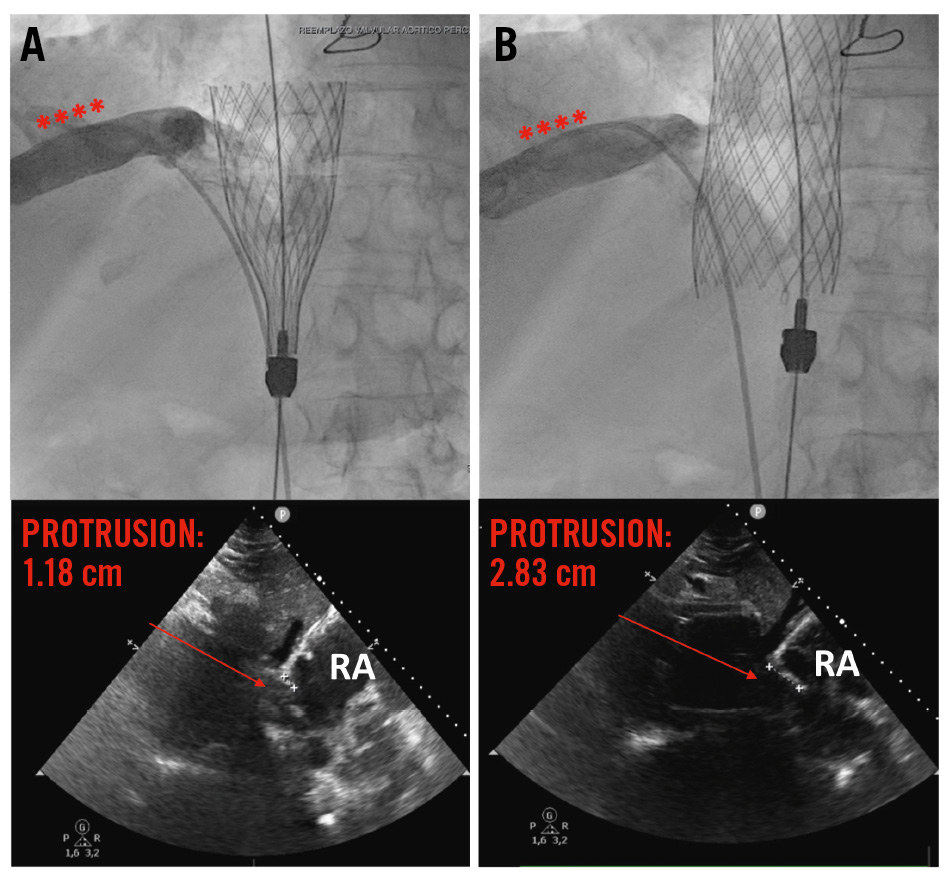
Figure 3. Inferior vena cava TricValve system prosthesis implantation. A) The red asterisks indicate the suprahepatic vein (anatomical landmark); below, the transthoracic echocardiogram showing adequate right atrium protrusion of 1.18 cm. B) IVC “pop-up”; below, the transthoracic echocardiogram showing a very high right atrium protrusion of 2.83 cm. IVC: inferior vena cava; RA: right atrium
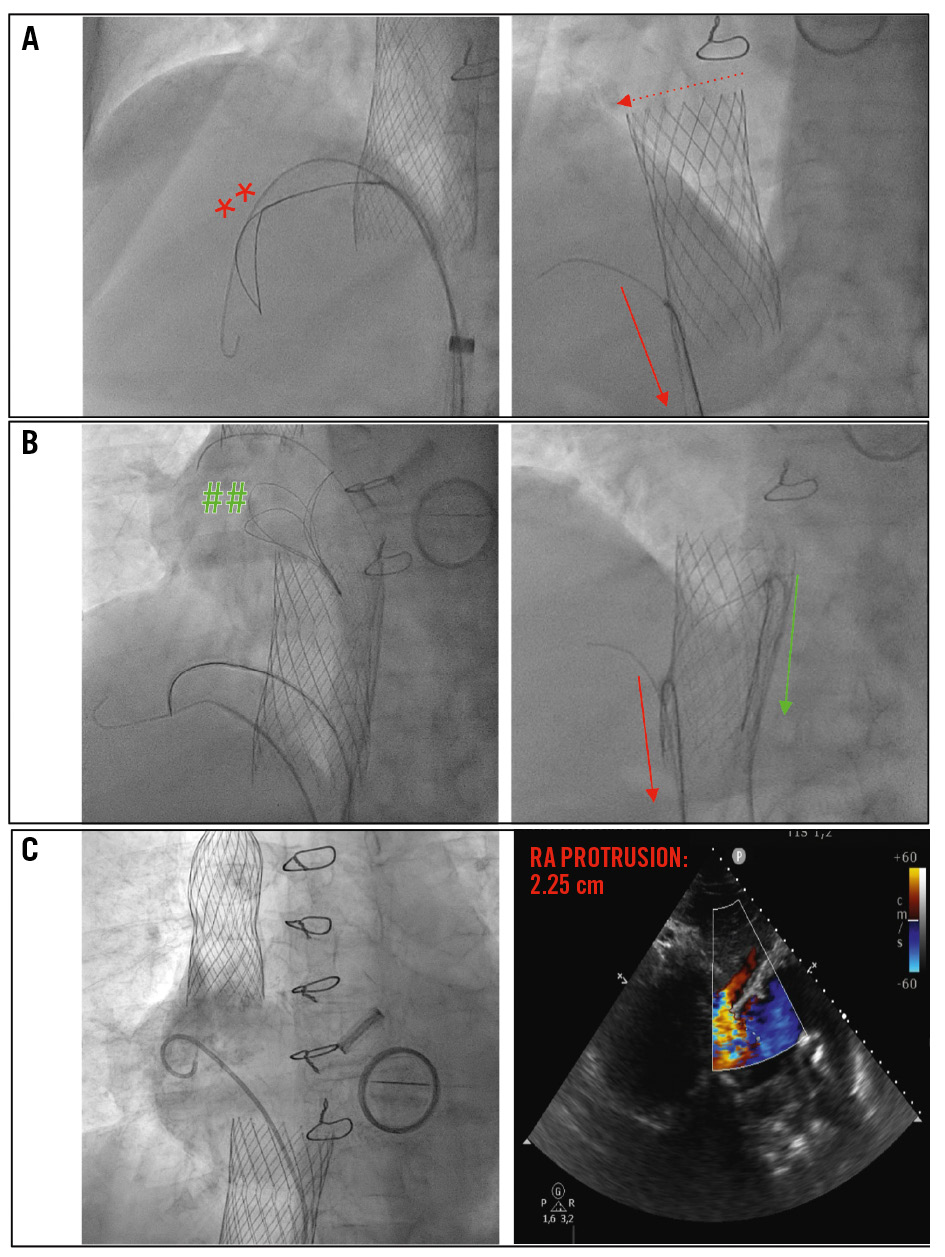
Figure 4. Management of IVC “pop-up” with snaring technique. A) Repositioning the prosthesis using a single snare (Amplatz Goose Neck – red asterisks) from the suprahepatic vein that resulted primarily in device tilting (red arrows); (B) the double-snare strategy using an Amplatz Goose Neck in the suprahepatic vein and an EN Snare (green ##). Traction was applied from two different positions and directions (green and red arrows). Simultaneous traction enabled repositioning of the prosthesis. C) Successful result with RA protrusion of 2.25 cm, no paravalvular leakage, and patent suprahepatic vein. RA: right atrium
Discussion
Our case illustrates a rare but important complication of TricValve system implantation: upward migration of the IVC prosthesis into the RA, followed by its prompt recognition and successful transcatheter management (Visual Summary).
CAVI has emerged as an alternative treatment for patients with severe TR who are not suitable candidates for surgery or transcatheter leaflet-based therapies.2 The TricValve system is the first European conformity (CE)-approved CAVI device consisting of 2 dedicated self-expanding nitinol stents with bovine pericardial leaflets implanted in the IVC and SVC to abolish the backflow responsible for systemic venous congestion.4 It has been shown to be safe and effective in relieving congestion and to significantly improve quality-of-life metrics at 6 and 12 months in patients with NYHA Functional Class III or IV and severe TR with right HF.46
Although the TricValve system is conceptually straightforward, optimal device positioning remains critical for procedural success. Malpositioning or migration of the IVC prosthesis represent challenging complications, particularly when cranial migration into the RA occurs. This may be related to insufficient anchoring, suboptimal alignment, or the complex interplay between venous compliance and right atrial dynamics.23
Prevention of device migration during CAVI is key. Preprocedural tomography is essential to identify challenging IVC anatomies, including severe dilatation, short landing zones, and unfavourable relationships with the suprahepatic veins. Adequate device sizing is crucial, particularly considering that patients with severe TR often present with variable volume status, which may significantly affect IVC dimensions and, consequently, device selection. Furthermore, precise deployment at the cavo-atrial junction with controlled release is critical to ensure stable anchoring and minimise the risk of migration.5
It is important to note that our patient’s IVC measurements fell within a “grey zone”, in which both 31 mm and 35 mm prostheses could have been considered (Figure 2).6 In such cases, optimal device selection and degree of oversizing can be particularly challenging. We believe that the use of a 31 mm prosthesis may have contributed to the subsequent migration into the RA, due to insufficient oversizing for adequate anchoring. Moreover, the presence of some longitudinal variability in the IVC (27 to 33 mm) (Figure 2) may have resulted in heterogeneous radial force distribution, predisposing the prosthesis to inadequate anchoring and cranial migration. No other technical issues were identified that could have contributed to this. Anatomical landmarks were clearly recognised, and deployment was performed in a slow and controlled manner with appropriate tension release.
In this case, significant cranial migration of the IVC valve resulted in marked protrusion into the RA and significant paravalvular leakage. While a certain degree of protrusion is expected (<15 mm),5 excessive displacement may compromise device function, increase the risk of embolisation, or interfere with adjacent structures. Therefore, prompt and effective correction is essential. Initial attempts using a single-snare technique (Amplatz Goose Neck) were unsuccessful and primarily resulted in device tilting, highlighting the limitations of unidirectional traction in controlling prosthesis orientation. The implementation of a double-snare strategy (EN Snare) allowed the application of multidirectional forces, providing improved control over both axial alignment and positional stability. This approach enabled gradual and controlled repositioning of the valve into a more desirable and favourable position without inducing further instability.
This case illustrates several important technical considerations. First, careful attention to anatomical landmarks and deployment technique are essential to minimise the risk of malpositioning. Second, when device migration occurs, understanding the underlying mechanism is key to selecting an effective bailout strategy. Finally, the double-snare technique represents a valuable and reproducible option for managing complex malpositioning scenarios, particularly when single-snare manoeuvres fail.
Conclusions
Upward migration of an IVC prosthesis during TricValve system implantation is an uncommon but manageable complication. A double-snare technique provides an effective percutaneous solution for retrieving and repositioning the device, ensuring procedural success without surgical intervention.
Impact on daily practice
TricValve system implantation is increasingly performed in patients with advanced tricuspid regurgitation and limited therapeutic options. Awareness of potential complications, such as the upward migration of a prosthesis, is essential for interventional cardiologists. This case demonstrates that percutaneous snare-based techniques, particularly those using a double-snare approach, can effectively resolve device malpositioning. Operators should be familiar with these bailout strategies and ensure that appropriate tools are available during the procedure. Prompt recognition through angiography and transthoracic echocardiography and decisive management are key to achieving optimal outcomes in complex structural interventions.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflict of interest statement
The authors have no conflicts of interest to declare.