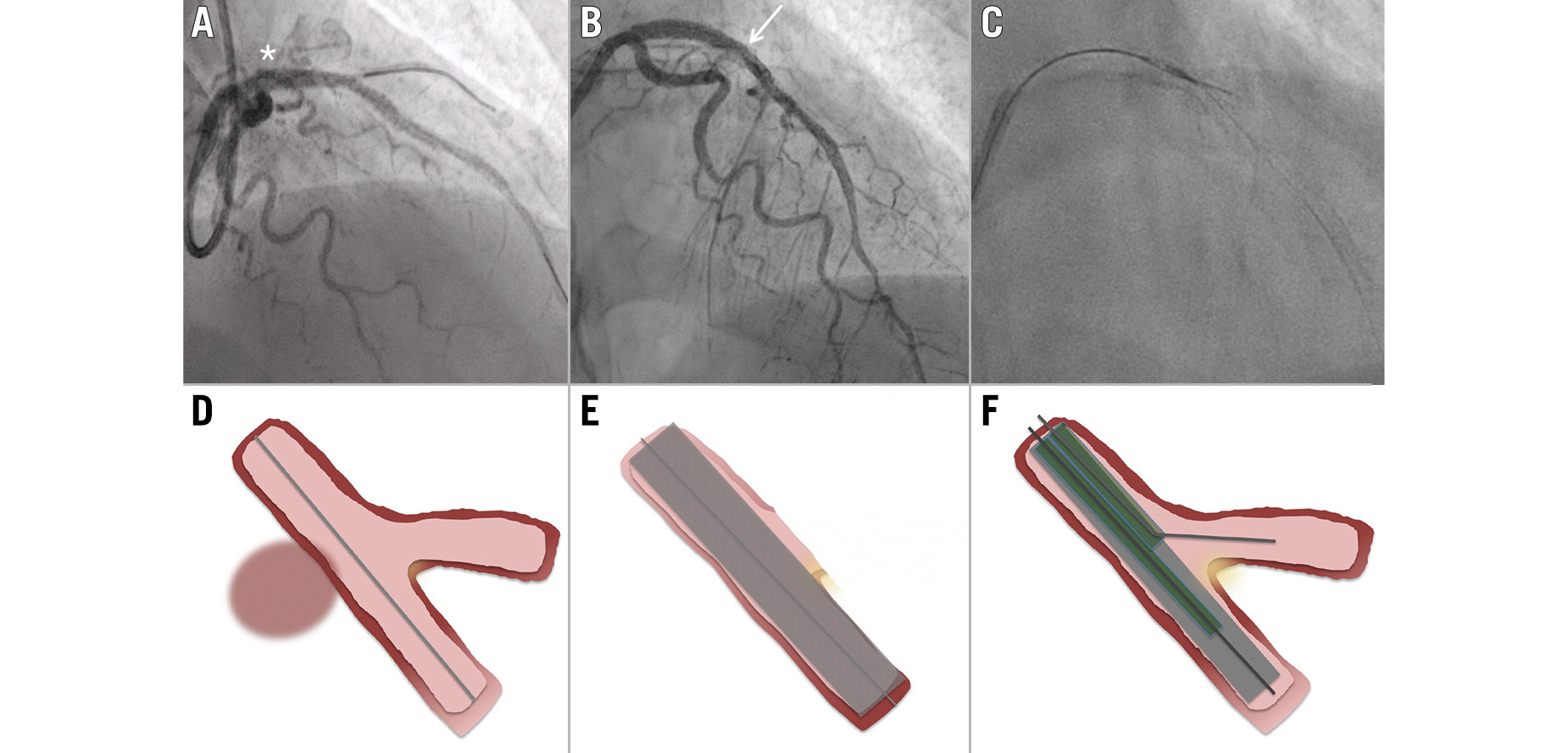
A) Coronary angiography demonstrating Ellis type III perforation (asterisk) requiring (B) covered stent implantation across a bifurcation with resultant side branch occlusion (arrow), followed by (C) controlled fenestration of the covered stent using a high tip-load guidewire via a dual lumen microcatheter. D-F) Schematic illustration of the key procedural steps corresponding to A-C.
Learning objectives
- Coronary perforation involving bifurcation lesions may require covered stent implantation across a side branch to achieve haemostasis.
- Side branch occlusion following covered stent deployment can be treated using controlled fenestration with a dual lumen microcatheter and high tip-load guidewire.
- Excimer laser therapy for drug-eluting stent in-stent restenosis adjacent to covered stents is feasible when performed with guide extension catheter protection.
Coronary artery perforation is a rare but life-threatening complication of percutaneous coronary intervention (PCI), with increasing incidence in complex, calcified interventions.1 Covered stents are often required for its definitive management but may compromise side branch flow in bifurcation lesions. This case demonstrates a reproducible technique to restore side branch flow following covered stent implantation across a bifurcation − a rare but significant challenge in complex PCI.
Case presentation
A 64-year-old female with a history of type 1 diabetes mellitus and asthma presented with a non-ST-segment elevation myocardial infarction (NSTEMI). Peak high-sensitivity troponin was 286 ng/L, and transthoracic echocardiography demonstrated preserved left ventricular systolic function.
Coronary angiography via 6 Fr right radial access revealed severe calcified disease in the proximal to mid-left anterior descending artery (LAD) with acute occlusion of the first diagonal branch (Figure 1A, Moving image 1). The left circumflex and right coronary arteries were unobstructed.
The diagonal branch was wired, predilated using a 2.5 mm non-compliant balloon (NCB) and treated with a 2.5×20 mm drug-coated balloon (DCB). The LAD underwent lesion preparation with a 2.5 mm NCB, a 2.5 mm scoring balloon (Scoreflex [OrbusNeich]), and a 3.0×12 mm Shockwave intravascular lithotripsy catheter (Shockwave Medical) (Figure 1B). Two drug-eluting stents (DES; XIENCE [Abbott]) were deployed in the LAD: a 3.0×28 mm stent distally and a 3.5×28 mm stent proximally, followed by graded post-dilation with 3.25 mm and 3.75 mm NCBs. Subsequent angiography demonstrated loss of flow in the diagonal branch (Figure 1C, Moving image 2).
The diagonal was rewired, and kissing balloon inflation (KBI) was performed using a 2.0 mm semicompliant balloon in the diagonal and a 3.0 mm NCB in the LAD (Figure 2A). This restored partial flow; however, subsequent angiography revealed a proximal LAD Ellis type III perforation (Figure 2B, Moving image 3).
Immediate balloon tamponade was performed with prolonged inflation of a 3.75 mm NCB (Figure 2C), during which the patient remained haemodynamically stable. However, upon balloon deflation, there was persistent contrast extravasation accompanied by haemodynamic instability, prompting deployment of a 3.5×20 mm PK Papyrus covered stent (Biotronik) proximal to the diagonal bifurcation, followed by post-dilation with a 3.75 mm NCB. Evidence of ongoing leakage despite further balloon tamponade (Moving image 4) necessitated placement of a second 3.0×20 mm covered stent across the diagonal origin, overlapping the first covered stent. This successfully sealed the perforation but resulted in occlusion of the diagonal branch (Moving image 5), with subsequent chest pain and dynamic lateral ST-segment depression on electrocardiography.
An NHancer Rx dual lumen microcatheter (IMDS) was advanced over the LAD wire. There was minimal residual filling of the occluded diagonal branch, and initial attempts to cross the covered stent membrane using a Fielder XT-A, and subsequently a Confianza Pro 12 (both Asahi Intecc), were unsuccessful. Fenestration was ultimately achieved using prior angiographic runs as a roadmap and maintaining consistent fluoroscopic projections; a high tip-load coronary guidewire (ASAHI Gaia Second [Asahi Intecc]) was delivered through the side port, successfully gaining access to the diagonal branch (Visual Summary, Figure 3A, Moving image 6). KBI was performed, but flow remained compromised, so T and protrusion (TAP) stenting was carried out using a 2.0×25 mm stent (Supraflex Cruz [SMT]) (Figure 3B). Final angiography demonstrated complete sealing of the perforation and restoration of Thrombolysis in Myocardial Infarction 3 flow in the diagonal branch (Figure 3C, Moving image 7).
The patient did not develop a significant pericardial effusion during the procedure. However, her postprocedural course was complicated by access site compartment syndrome, which was treated successfully with fasciotomy prior to discharge.
At 9-month follow-up, the patient presented with stable angina. Repeat angiography demonstrated focal in-stent restenosis within the DES distal to the covered stents (Figure 4A), and an intravascular ultrasound (IVUS) confirmed focal underexpansion (Figure 4B). Despite treatment with 3.25 mm high-pressure NCB dilation and repeat 3.5 mm intravascular lithotripsy, expansion remained suboptimal.
The lesion was subsequently treated with excimer laser coronary atherectomy (80 Hz, 12,000 pulses), delivered through a guide extension catheter which was positioned proximally to protect the covered stents (Figure 4C). This achieved improved stent expansion, and adjunctive treatment with a 3.5×30 mm DCB resulted in an excellent final angiographic outcome (Figure 4D).
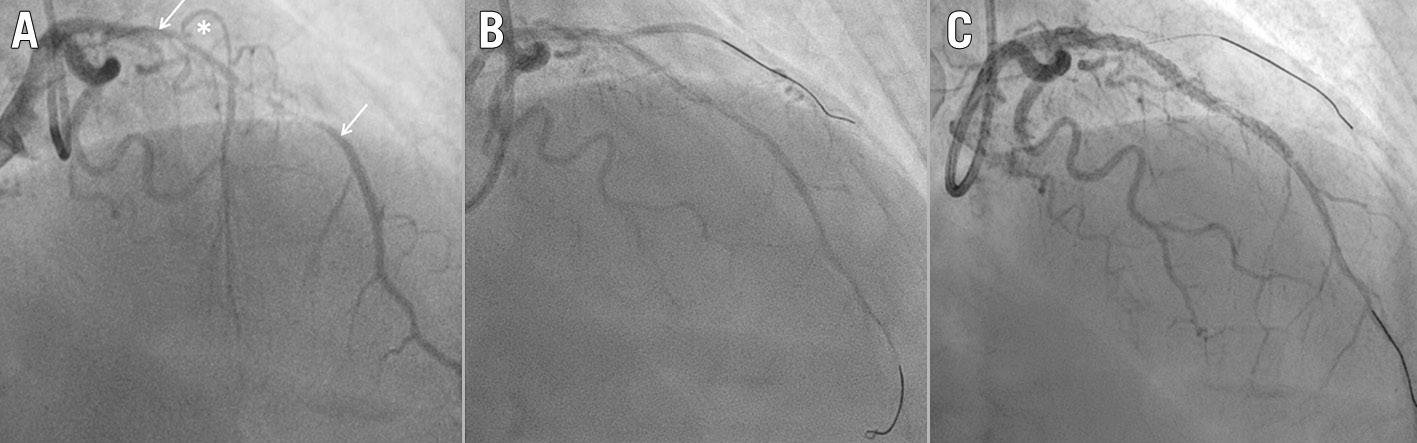
Figure 1. Coronary angiography. A) Baseline angiogram demonstrating severe calcified disease in the proximal to mid-left anterior descending artery (arrows) with occlusion of the first diagonal branch (asterisk). B) Angiographic appearance following lesion preparation. C) Angiogram following stent implantation demonstrating loss of diagonal branch flow.
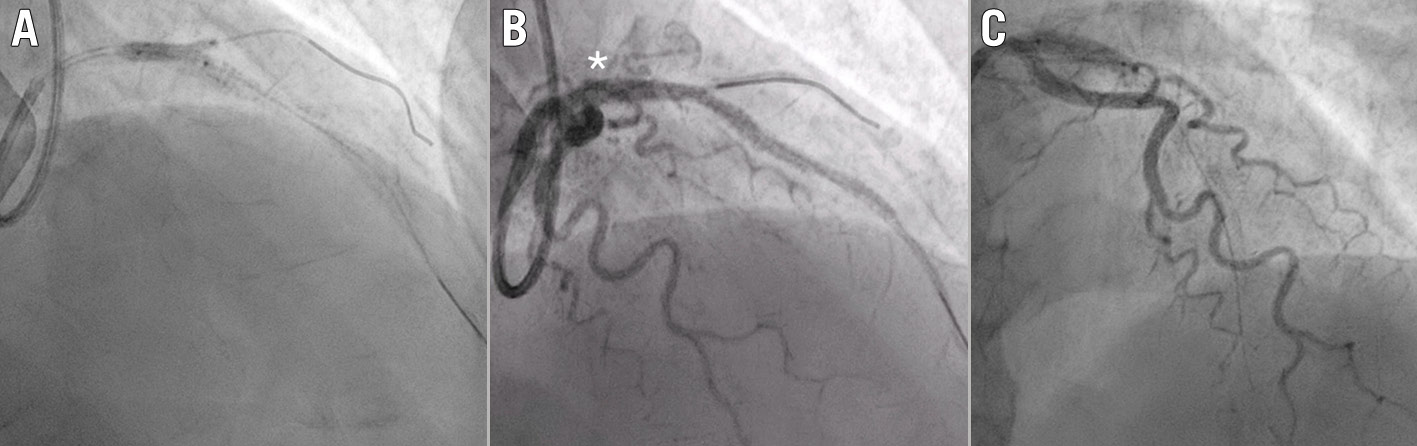
Figure 2. Procedural angiography. A) Kissing balloon inflation in the left anterior descending artery (LAD) and diagonal branch. B) Proximal LAD Ellis type III perforation (asterisk). C) Balloon tamponade of the proximal LAD.
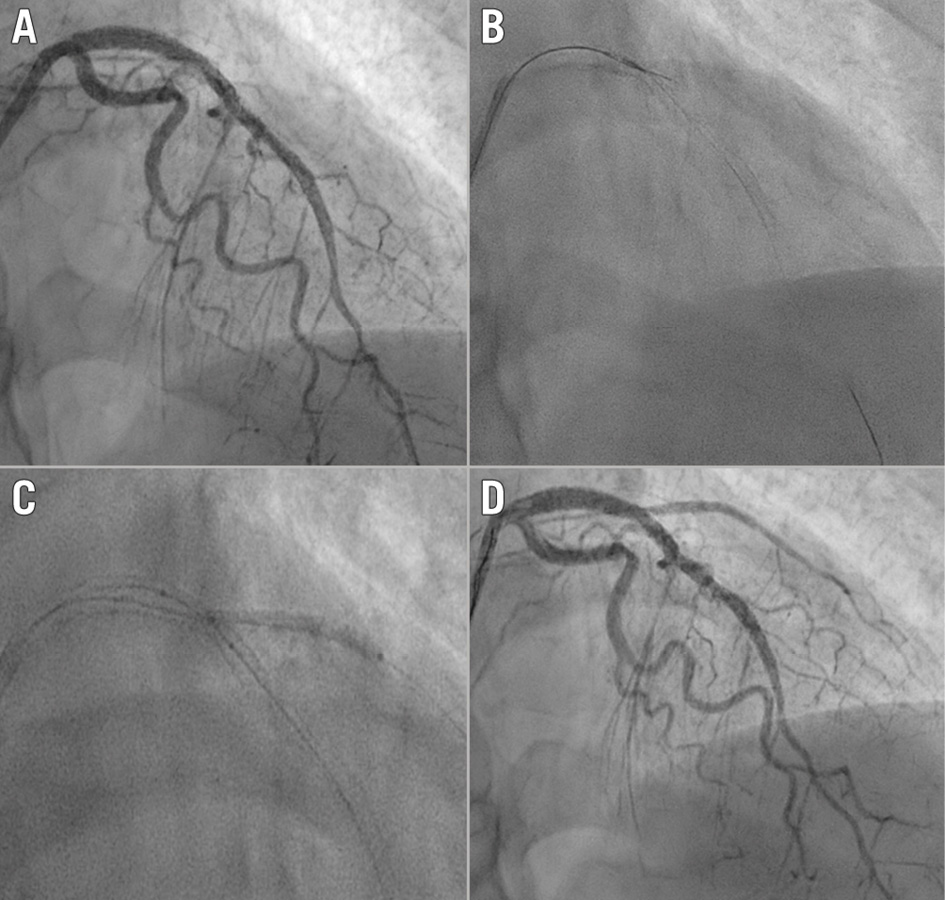
Figure 3. Bifurcation rescue following covered stent implantation. A) Covered stent deployed across the bifurcation with occlusion of the diagonal branch. B) Dual lumen microcatheter with a high tip-load guidewire advanced through the side port, fenestrating the covered stent membrane into the diagonal branch. C) Side branch stenting using the T and protrusion technique. D) Final angiographic result demonstrating complete sealing of the perforation and restoration of flow in the diagonal branch.
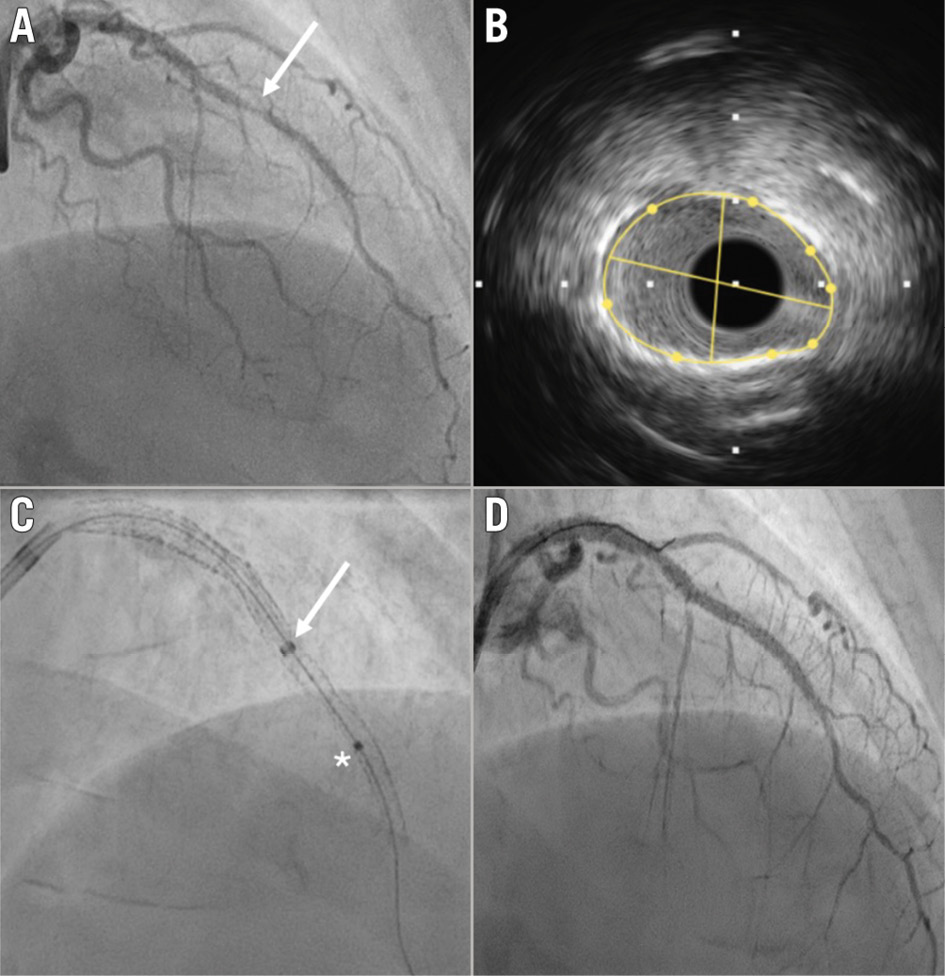
Figure 4. Follow-up angiography and intravascular imaging. A) Focal drug-eluting stent in-stent restenosis (arrow) distal to the covered stents. B) Intravascular ultrasound demonstrating an underexpanded segment with a minimal stent area of 4.21 mm². C) Excimer laser coronary atherectomy (asterisk) delivered through a guide extension catheter (arrow) positioned to protect the covered stents. D) Final angiographic result following lesion modification and drug-coated balloon treatment.
Discussion
Coronary artery perforation is an uncommon but potentially catastrophic complication of PCI, with an incidence of approximately 0.2-0.6%; this risk increases with the treatment of complex and heavily calcified lesions requiring aggressive lesion modification strategies.2
Ellis type III perforations represent the most severe form, associated with significant extravasation and risk of tamponade, and they require immediate recognition and prompt management. Balloon tamponade remains the first-line stabilisation strategy; however, persistent leakage necessitates definitive sealing, most commonly with covered stent implantation.3
Covered stents, including the PK Papyrus device, are highly effective in achieving haemostasis but are inherently limited by their impermeable membrane, which frequently compromises side branch flow when deployed across bifurcations.3 This presents a significant therapeutic challenge, particularly when the side branch supplies viable myocardium.
Fenestration of covered stents to restore side branch flow has been described in only a limited number of case reports. The technique was first demonstrated as a feasible bailout strategy using stiff or high-penetration guidewires to create a controlled defect in the stent membrane, allowing reaccess to the side branch.4 Subsequent reports have confirmed its utility in selected cases, predominantly involving left main or major bifurcation anatomy.5 Importantly, Lindner et al highlighted that only a small number of cases involving bifurcation perforations treated with covered stent fenestration and two-stent strategies have been reported, underscoring the rarity of this approach and the absence of standardised techniques.6
Various strategies may be considered to increase the chances of successful fenestration through the covered stent into the side branch. Consideration was given to leaving a jailed guidewire in the side branch as a marker; however, this strategy was not pursued in this case. Covered stents incorporate a polymer membrane that may be more susceptible to mechanical disruption, and withdrawal of a jailed guidewire carries a potential risk of focal traction on the stent structure, which could result in “cheese-wiring” of the membrane and compromise of the sealing effect. An alternative strategy would be to stent the side branch prior to placement of the covered stent to provide a clear target for reaccess; however, the haemodynamic instability in this case was deemed prohibitive.
In the present case, the use of prior angiographic runs as a roadmap, with consistent fluoroscopic projections, in conjunction with a dual lumen microcatheter, facilitated controlled and directed reaccess to the side branch. The selection of a high tip-load chronic total occlusion guidewire (ASAHI Gaia Second) enabled effective penetration of the covered stent membrane. This combination provides a reproducible and controlled method for fenestration, minimising the risk of uncontrolled disruption or reperforation. Following successful re-entry, the use of KBI and TAP stenting allowed restoration of side branch patency while maintaining integrity of the perforation seal. This approach adapts established bifurcation PCI principles to a complex bailout scenario but requires a careful case-by-case assessment to balance the benefits of side branch revascularisation against the risk of reperforation during fenestration.
The need for subsequent reintervention highlights the importance of adequate lesion preparation to facilitate optimal stent expansion, particularly in calcified lesions. IVUS-guided assessment confirmed underexpansion as the mechanism of restenosis, and excimer laser coronary atherectomy provided effective modification where conventional and lithotripsy-based strategies had failed. Although the acute perforation is expected to have healed at midterm follow-up, covered stents incorporate a non-porous polymer membrane (e.g. polyurethane or polytetrafluoroethylene), which is associated with delayed and potentially incomplete endothelialisation compared with conventional DES. As a result, the stent surface and membrane may remain susceptible to mechanical or thermal injury. Delivery of excimer laser energy in close proximity to a covered stent therefore raises a theoretical risk of membrane disruption or alteration of the stent structure, with potentially unpredictable consequences. In this case, a guide extension catheter was advanced to cover the proximal segment of the covered stent, thereby limiting direct laser exposure and providing a controlled environment for energy delivery. While this represents a precautionary approach and is not routinely required, it may be considered in selected cases in the absence of robust data regarding laser use adjacent to covered stents.
Conclusion
Fenestration and TAP stenting to re-establish side branch flow is a feasible bailout strategy after covered stent deployment in bifurcation perforation cases.
Impact on daily practice
Covered stents used to treat coronary perforation may compromise side branch flow in bifurcation lesions. Fenestration using a dual lumen microcatheter and high tip-load guidewire provides a reproducible method to restore side branch perfusion while maintaining haemostasis in selected cases. Careful follow-up and intravascular imaging-guided optimisation, if clinically indicated, is important to optimise long-term outcomes.
Conflict of interest statement
The authors have no conflicts of interest to declare.