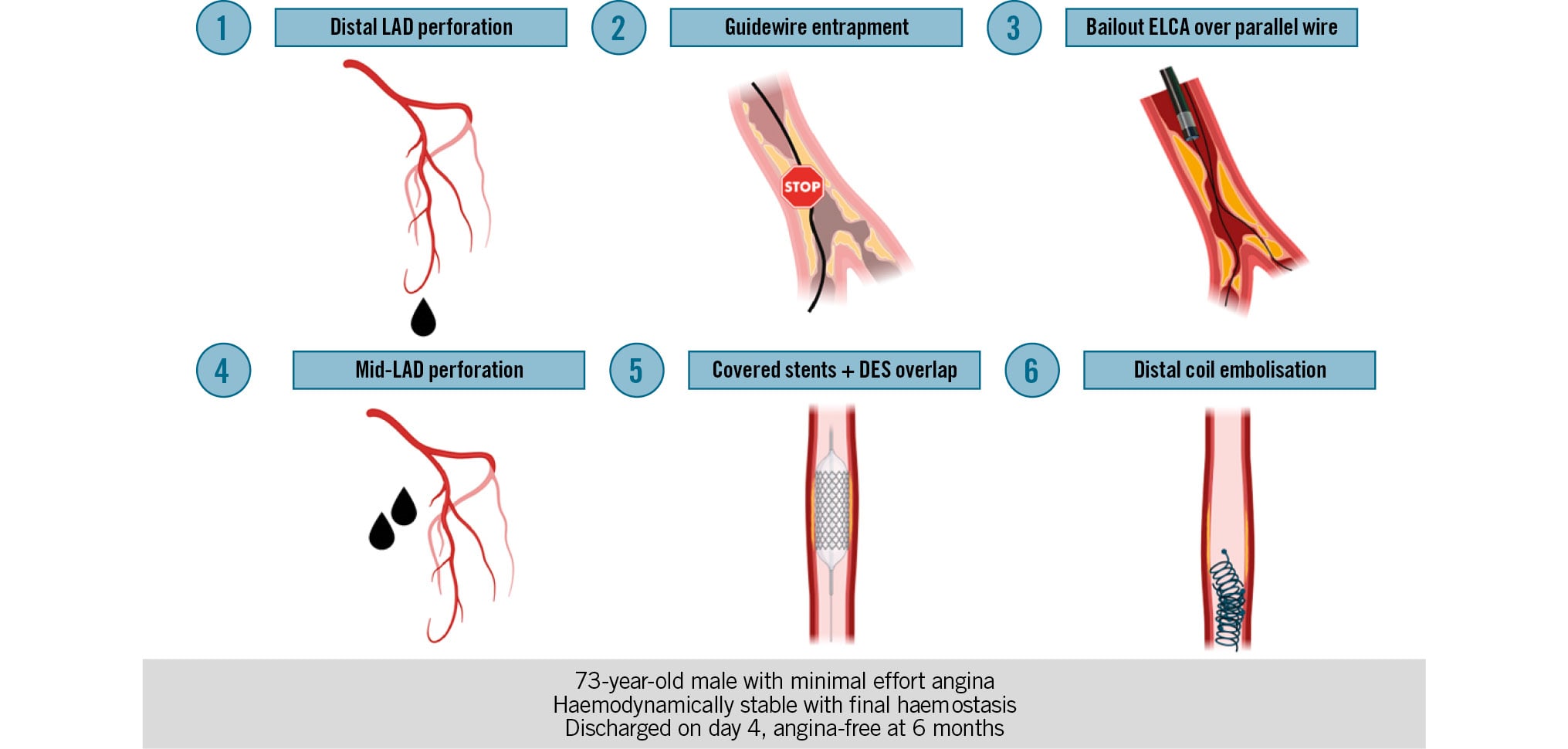
Procedural complication cascade and stepwise bailout management. DES: drug-eluting stent; ELCA: excimer laser coronary atherectomy; LAD: left anterior descending
Learning objectives
- To recognise guidewire entrapment early during percutaneous coronary intervention of severely calcified coronary lesions
- To understand how device uncrossability, distal perforation, and guidewire entrapment may interact in a complication cascade
- To describe the role of bailout excimer laser coronary atherectomy for guidewire release when conventional retrieval strategies fail
Severely calcified uncrossable coronary lesions remain a major challenge in percutaneous coronary intervention (PCI).12 In this setting, procedural complications may evolve into a cascade of interrelated events requiring early recognition and stepwise bailout management.
Guidewire entrapment is an uncommon but potentially serious PCI complication, typically encountered in heavily calcified, tortuous, or chronic total occlusion (CTO) lesions. When conventional retrieval strategies fail, treatment options become limited and may include advanced plaque modification techniques or surgery.34 Recent case reports have suggested a potential role for excimer laser coronary atherectomy (ELCA) as a bailout strategy for guidewire release in severely calcified vessels.56
We report a case of PCI of a severely calcified mid-left anterior descending artery (LAD) chronic subocclusion complicated by guidewire entrapment (solved with bailout ELCA), and a combination of distal- and mid-LAD perforations managed with covered stents and distal coil embolisation.
Case summary
A 73-year-old male with metastatic pancreatic adenocarcinoma under active treatment was referred for invasive management due to minimal effort angina. Coronary angiography performed at another centre had shown diffuse severe coronary calcification, with a chronic subocclusion of the mid-LAD, a severely calcified lesion in the left circumflex artery, and moderate disease of the right coronary artery (Figure 1A-Figure 1B-Figure 1C, Moving image 1). A previous revascularisation attempt had failed because the LAD lesion could not be wired.
A new PCI attempt to the LAD was performed via right radial access using a 6 Fr Extra backup (EBU) 3.5 (Medtronic) guiding catheter. Initial attempts to cross the lesion with SION blue (Asahi Intecc) and FIGHTER (Boston Scientific) guidewires were unsuccessful. A Gladius EX14 (Asahi Intecc) guidewire eventually crossed the lesion, supported by a Caravel microcatheter (Asahi Intecc). After predilatation with 1.0 mm and 1.5 mm balloons (Moving image 2), a Caravel microcatheter was advanced distally, and the Gladius EX14 was exchanged for a SION blue ES (Asahi Intecc). Optical coherence tomography was then attempted but could not cross the lesion. Repeat attempts to advance small balloons were also unsuccessful, and no device could subsequently cross the lesion, despite support escalation with a Telescope guide extension catheter (Medtronic). During this phase, a distal LAD perforation occurred (Figure 2A, Moving image 3). A Caravel microcatheter was then advanced over the SION blue ES in an attempt to reach the distal vessel and deliver coils, but again, device crossing was impossible. At that stage, guidewire entrapment at the level of the severely calcified mid-LAD was suspected. Several bailout manoeuvres were attempted, including traction, telescoping support, and balloon-assisted techniques, all without success. A second SION blue guidewire was advanced in parallel; however, neither balloons nor microcatheters could cross the lesion over either of the two guidewires.
Given the persistent device uncrossability and failure of conventional retrieval manoeuvres, bailout ELCA was performed over the second, non-entrapped guidewire using a Vitesse 0.9 mm rapid exchange disposable catheter (Spectranetics) with saline injection (Figure 2B, Moving image 4). Laser energy was delivered at 40 mJ/mm2 and 40 Hz in 5 runs over 25 seconds (1,000 pulses), successfully releasing the entrapped guidewire (Moving image 5), but this was immediately followed by a second, mid-LAD Ellis type III perforation (Figure 2C, Moving image 6). Two overlapping PK Papyrus 2.5×20 mm covered stents (Biotronik) were implanted to seal the mid perforation, followed by a proximal overlap with an Orsiro Mission 3.0×30 mm drug-eluting stent (Biotronik) (Figure 3A, Moving image 7). Protamine was not administered. A microcatheter was then advanced distally, and two coils were implanted, achieving final haemostasis of the distal perforation (Figure 3B). The final angiogram showed the successful sealing of both perforations (Figure 3C, Moving image 8). Throughout the procedure, the patient remained haemodynamically stable, with no significant pericardial effusion. He was discharged home on day 4. At 6-month follow-up, he remained free from angina and continued his oncological treatment.
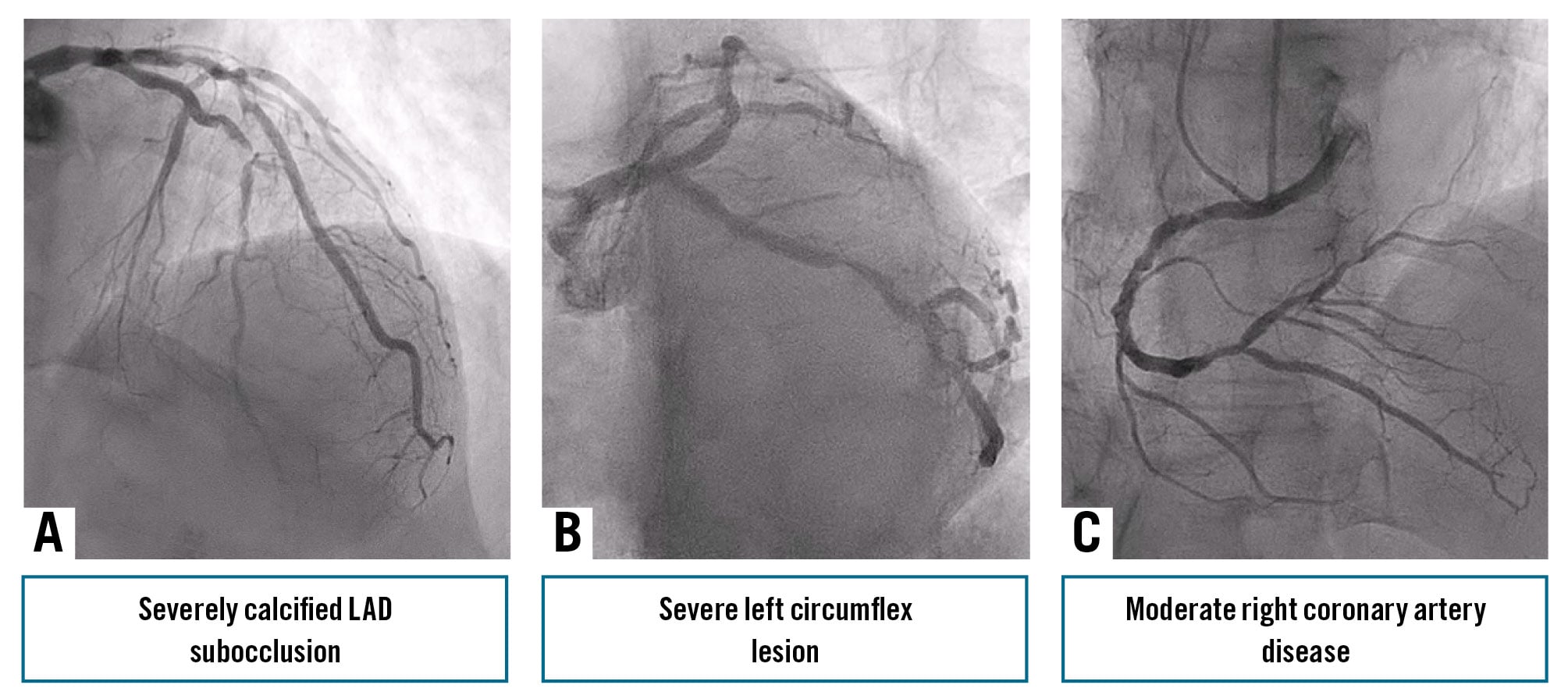
Figure 1. Baseline coronary angiogram. A, B) Diffuse severe left coronary calcification, with mid-LAD chronic subocclusion and a severely calcified left circumflex lesion. C) Moderate right coronary artery disease. LAD: left anterior descending
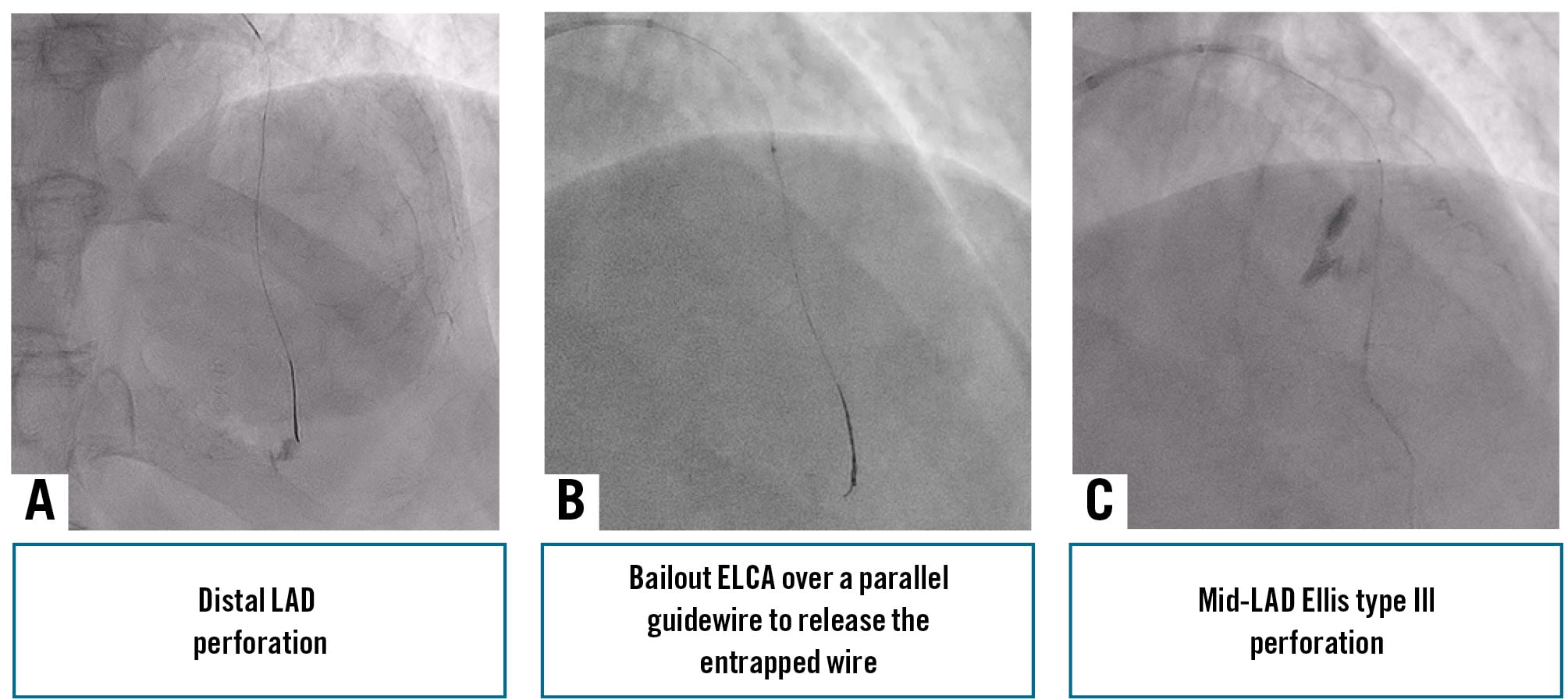
Figure 2. Procedural complication cascade. A) Distal LAD perforation. B) Bailout ELCA over a parallel guidewire for guidewire entrapment. C) Mid-LAD Ellis type III perforation after ELCA. ELCA: excimer laser coronary atherectomy; LAD: left anterior descending
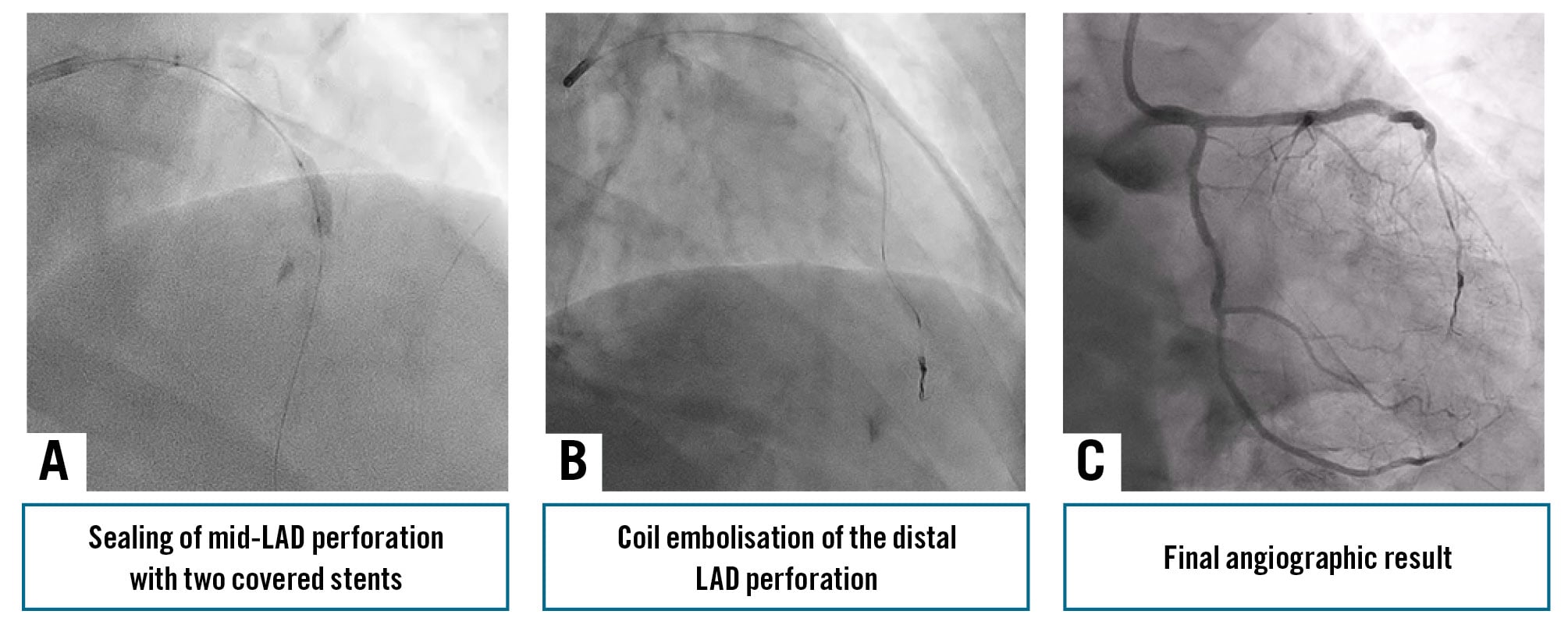
Figure 3. Bailout treatment and final angiographic result. A) Mid-LAD sealing with two covered stents and proximal drug-eluting stent overlap. B) Distal coil embolisation. C) Final angiogram showing successful sealing of both perforations. LAD: left anterior descending
Discussion
This case illustrates how PCI of a severely calcified CTO-like LAD lesion can rapidly evolve from a crossing problem into a complication cascade (Visual Summary). The lesion combined several unfavourable features, including chronic subocclusion, marked calcific burden, vessel tortuosity, and a previously failed revascularisation attempt. After successful guidewire crossing and initial predilatation with a 1.5 mm balloon, no other device was able to cross the lesion, including intravascular imaging catheters, repeat small balloons, and subsequent rescue devices. This distinction is important because in heavily calcified lesions, procedural failure and procedural complications often arise from the same anatomical substrate.
Guidewire entrapment is an uncommon but potentially serious complication of PCI. It has been associated with heavily calcified and tortuous vessels, particularly when repeated manipulation is required in resistant anatomy.3 Once entrapment occurs, operators should avoid uncontrolled traction, as this may worsen wire deformation, elongation, or fracture and make subsequent retrieval more difficult.4 Several percutaneous strategies have been described, including guidewire rotation or traction, advancement of a microcatheter, balloon, or guide extension catheter over the wire, parallel wire techniques, snaring in the case of fracture, and, in selected circumstances, surgical extraction.4 In our case, the conventional percutaneous options were limited not only by the entrapment itself, but also by the persistent inability to cross the lesion with microcatheters or balloons, even after support escalation.
Another important message from this case is the need to recognise complication cascades early. A distal LAD perforation occurred during manipulation of an extra support wire in a severely calcified and resistant vessel. Notably, after initial predilatation, the lesion became completely device-uncrossable, preventing the delivery of imaging catheters, repeat balloons, and later, coil- or retrieval-related equipment. Given the absence of intravascular imaging at that stage, the exact mechanism remains uncertain. One possible explanation is that the initial balloon dilatation modified the calcified segment in a way that may have further increased lesion uncrossability and contributed to guidewire entrapment. In such scenarios, successful management depends not only on solving each individual problem, but on understanding when the procedural strategy needs to change altogether.
This case also highlights the need for particular caution when using extra support wires in heavily calcified or tortuous distal anatomy. Although these wires are often required to achieve lesion crossing in complex PCI, they may increase the risk of distal vessel injury when advanced into small, resistant, or sharply angulated segments. In the present case, distal perforation may have resulted from a combination of hostile distal anatomy, the position of the guidewire transition zone, and forward displacement of the guidewire during traction on the entrapped system.
ELCA represented the key bailout strategy in our case and was chosen only after conventional retrieval manoeuvres had failed. At that stage, plaque modification represented one of the last percutaneous options for managing guidewire entrapment,4 but alternative techniques were not feasible. Intravascular lithotripsy was not possible because further balloon delivery could no longer be achieved after initial predilatation. Rotational and orbital atherectomy were also unsuitable because a microcatheter could not be advanced for exchange to a dedicated atherectomy wire, while direct wiring with such a wire would likely have been challenging. By contrast, ELCA was able to be delivered over the existing 0.014" guidewire and allowed proximal plaque modification without lesion crossing. Beyond guidewire entrapment, ELCA is an established and generally safe tool in complex calcified PCI, with recognised roles in both uncrossable and undilatable lesions.12789 More recently, its use has also been extended to the retrieval of entrapped guidewires in heavily calcified vessels. Li et al reported the successful liberation of an entrapped guidewire during CTO PCI after the failure of conventional methods,5 while Asselin et al described the successful retrieval of an isolated entrapped guidewire in a severely calcified vessel using ELCA with saline injection.6 Our case is consistent with these reports in supporting the feasibility of laser-assisted wire liberation, but differs in some important respects, as the lesion was extremely calcified and tortuous and had already undergone balloon-based calcium modification. These features are important when interpreting the subsequent perforation, although its exact mechanism remains uncertain. A plausible explanation is that laser application in an already injured, heavily calcified vessel contributed to perforation in a vulnerable segment. To minimise complications, ELCA in this setting should be reserved for selected bailout cases, with cautious energy delivery and avoidance of aggressive advancement. In this context, ELCA was crucial to achieve wire liberation after the failure of conventional retrieval strategies and likely avoided the need for urgent surgery. ELCA remains a highly useful option in selected cases of guidewire entrapment, but its use in this setting should be reserved for situations in which standard techniques have failed, and perforation-management tools are immediately available, including covered stents, embolisation materials, and haemodynamic support if needed. This case reflects a highly selected bailout scenario and should not be generalised to routine practice. It illustrates a potential rescue strategy when standard options have failed.
Conclusions
PCI of severely calcified CTO-like LAD lesions may trigger a rapid complication cascade linking distal perforation, device uncrossability, and guidewire entrapment. ELCA can be an effective bailout strategy for guidewire entrapment. Careful wire handling and procedural control remain key to a favourable outcome.
Impact on daily practice
In severely calcified and uncrossable coronary lesions, operators should be aware that device uncrossability, guidewire entrapment, and distal perforation may occur as interconnected complications rather than isolated events. Early recognition of this evolving scenario is essential. Particular caution is required when manipulating extra support guidewires in tortuous distal anatomy. When conventional retrieval strategies fail, excimer laser coronary atherectomy may represent an effective bailout option, provided that perforation-management tools, including covered stents and distal embolisation materials, are immediately available.
Consent statement
Written informed consent was obtained from the patient for publication of this case report.
Conflict of interest statement
M. Basile received a research grant from IHT. A. Jurado-Román is a proctor for Abbott, Boston Scientific, World Medica, and Philips; has received consulting fees from Boston Scientific and Philips; and has received speaker fees from Abbott, Boston Scientific, Shockwave Medical, Philips, and World Medica. The other authors have no conflicts of interest to declare.